
Abstract
Objective
International guidelines for the management of unruptured intracranial aneurysms (UIAs) recommend observation in aneurysms <10 mm due to the estimated low risk of rupture. The aim of our study was analyse the data of recently treated patients with ruptured cerebral aneurysms with the special focus on size and configuration in view of the frequency scale in a daily routine setting.
Methods
We reviewed the data of all patients with aneurysmal subarachnoid haemorrhage (SAH) during the last 24 months at our institution. Configuration and size of the aneurysms were measured. Clinical data were collected using the following classifications for analysis: Hunt and Hess (H&H), modified Rankin Scale (mRS) and Fisher classification.
Results
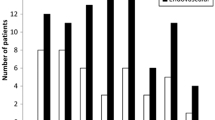
Data of 135 patients with aneurysmal SAH (98 women, 37 men; ratio 2.6:1) were analysed. Analysis showed that 19 aneurysms (14 %) were >10 mm (mean size, 19.2 mm) and 116 aneurysms (85.9 %) <10 mm (mean size, 6.2 mm). In total, 112 were categorised as berry-like configured aneurysms (n = 113 <10 mm, n = 3 >10 mm), 18 as multi-lobar (n = 16 <10 mm, n = 2 >10 mm) and 5 as fusiform (n = 4 <10 mm, n = 1, >10 mm).
Conclusion
Since the results of our study showed that the majority of the aneurysms are <10 mm (mean, 6.2 mm), it is justified to challenge the recommendations of the international guidelines in a daily routine setting. We believe that the published data are not convincing enough to play a guidance role in daily routine. Due to improving surgical and endovascular techniques with satisfying results and the high number of ruptured small aneurysms, we believe a change in attitude in management of small-sized aneurysms is needed. Further diagnostic models are needed to determine the risk of rupture of intracranial aneurysms properly to obtain adequate treatment for UIAs.




Similar content being viewed by others


References
Andaluz N, Zuccarello M (2008) Recent trends in the treatment of cerebral aneurysms: analysis of a nationwide inpatient database. J Neurosurg 108(6):1163
Bederson JB, Awad IA, Wiebers DO, Piepgras D, Haley EC Jr, Brott T, Hademenos G, Chyatte D, Rosenwasser R, Caroselli C (2000) Recommendations for the management of patients with unruptured intracranial aneurysms: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke 31(11):2742–2750
Burns JD, Brown RD Jr (2009) Treatment of unruptured intracranial aneurysms: surgery, coiling, or nothing? Curr Neurol Neurosci Rep 9(1):6–12
Chang HS (2006) Simulation of the natural history of cerebral aneurysms based on data from the International Study of Unruptured Intracranial Aneurysms. J Neurosurg 104(2):188–194
Connolly ES Jr, Solomon RA (1998) Management of symptomatic and asymptomatic unruptured aneurysms. Neurosurg Clin N Am 9(3):509–524
Horowitz M (2009) Guidelines for the surgical treatment of unruptured intracranial aneurysms: the first annual J. Lawrence Pool Memorial Research Symposium—controversies in the management of cerebral aneurysms. Neurosurgery 64(3):E577
International Study of Unruptured Intracranial Aneurysms Investigators (1998) Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med 339(24):1725–1733
Ishibashi T, Murayama Y, Urashima M, Saguchi T, Ebara M, Arakawa H, Irie K, Takao H, Abe T (2009) Unruptured intracranial aneurysms: incidence of rupture and risk factors. Stroke 40(1):313–316
Juvela S, Porras M, Poussa K (2008) Natural history of unruptured intracranial aneurysms: probability of and risk factors for aneurysm rupture. J Neurosurg 108(5):1052–1060
Komotar RJ, Mocco J, Solomon RA (2008) Guidelines for the surgical treatment of unruptured intracranial aneurysms: the first annual J. Lawrence pool memorial research symposium—controversies in the management of cerebral aneurysms. Neurosurgery 62(1):183–193
Lin N, Ho A, Gross BA, Pieper S, Frerichs KU, Day AL, Du R (2012) Differences in simple morphological variables in ruptured and unruptured middle cerebral artery aneurysms. J Neurosurg 117(5):913–919
Loewenstein JE, Gayle SC, Duffis EJ, Prestigiacomo CJ, Gandhi CD (2012) The natural history and treatment options for unruptured intracranial aneurysms. Int J Vasc Med 2012:898052
Nahed BV, DiLuna ML, Morgan T, Ocal E, Hawkins AA, Ozduman K, Kahle KT, Chamberlain A, Amar AP, Gunel M (2005) Hypertension, age, and location predict rupture of small intracranial aneurysms. Neurosurgery 57(4):676–683
Panigrahi M, Sanjay T, Reddy AK (2002) Unruptured intracranial aneurysms: review of natural history and recommended management strategies. Neurol India 50(Suppl):S115–S121
Raabe A, Seifert V, Schmiedek P, Steinmetz H, Bertalanffy H, Steiger HJ, Stolke D, Forsting M, American Heart Association; Section of Vascular Neurosurgery of the German Society of Neurosurgery (2002) Recommendations for the management of unruptured intracranial aneurysms. Zentralbl Neurochir 63(2):70–76
Petridis AK, Doukas A, Niu H, Barth H, Maslehaty H, Riedel C, Jansen O, Mehdorn HM (2011) Three dimensional rotational angiography in surgical planning of aneurysm clipping. Vasa 40(5):375–380
Raymond J, Guillemin F, Proust F, Molyneux AJ, Fox AJ, Claiborne JS, Meder JF, Rouleau I, Trial ON Endovascular Aneurysm Management (TEAM) Collaborative Group (2008) Unruptured intracranial aneurysms a critical review of the International Study of Unruptured Intracranial Aneurysms (ISUIA) and of appropriate methods to address the clinical problem. Interv Neuroradiol 14(1):85–96
Reith W, Grunwald IQ (2002) Nonruptured intracranial aneurysms: therapeutic recommendations. Radiologe 42(11):885–891
Sato K, Yoshimoto Y (2011) Risk profile of intracranial aneurysms: rupture rate is not constant after formation. Stroke 42(12):3376–3381
Sonobe M, Yamazaki T, Yonekura M, Kikuchi H (2010) Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke 41(9):1969–1977
UCAS Japan Investigators, Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, Hashimoto N, Nakayama T, Sakai M, Teramoto A, Tominari S, Yoshimoto T (2012) The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med 366(26):2474–2482
Wermer MJ, van der Schaaf IC, Algra A, Rinkel GJ (2007) Risk of rupture of unruptured intracranial aneurysms in relation to patient and aneurysm characteristics: an updated metaanalysis. Stroke 38(4):1404–1410
Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, Forbes GS, Thielen K, Nichols D, O’Fallon WM, Peacock J, Jaeger L, Kassell NF, Kongable-Beckman GL, Torner JC, International Study of Unruptured Intracranial Aneurysms Investigators (2003) Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 362(9378):103–110
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This important paper addresses well the controversy between the ISUIA recommendations followed by many, if not most, and daily clinical practice where most of the ruptured aneurysms are small in size. We analysed a series of 3,000 patients with ruptured aneurysms treated during the last 20 years, and in 66 % the size was smaller than 10 mm and, notably, in 14 % smaller than 5 mm. As the incidence of SAH in Finland (and Japan) for undefined reasons is 2–3 times higher than elsewhere, and people are living longer and healthier lives, we recommend unruptured aneurysms ≥3 mm to be treated in patients up to 70 years of age. Cessation of smoking and active treatment of hypertension is pertinent in all age groups.
Hanna Lehto
Mika Niemelä
Helsinki, Finland
H. Maslehaty and H. Ngando contributed equally to this study
Rights and permissions
About this article
Cite this article
Maslehaty, H., Ngando, H., Meila, D. et al. Estimated low risk of rupture of small-sized unruptured intracranial aneurysms (UIAs) in relation to intracranial aneurysms in patients with subarachnoid haemorrhage. Acta Neurochir 155, 1095–1100 (2013). https://doi.org/10.1007/s00701-013-1688-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-013-1688-y