
Abstract
Purpose
Cardiac sarcoidosis (CS) patients are at increased risk for sudden death. Isolated CS is rare and can be difficult to diagnose.
Methods
In this multicenter retrospective review, patients with CS and an implantable cardiac defibrillator (ICD) were identified.
Results
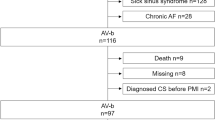
Of 235 patients with CS and ICD, 13 (5.5 %) had isolated CS, including 7 (3.0 %) with definite isolated CS (biopsy or necropsy-proven) and 6 (2.6 %) with suspected isolated CS based on a constellation of clinical, ECG, and imaging findings. Among 13 patients with isolated CS, 10 (76.9 %) were male, mean age was 53.8 ± 7.6 years, and mean left ventricular ejection fraction was 38.3 ± 16.5. Diagnosis was made by cardiac magnetic resonance (CMR) (n = 2), biopsy (n = 3), CMR and biopsy (n = 2), CMR and positron emission tomography (PET) (n = 2), PET (n = 1), late enhanced cardiac CT (n = 1), pathology at heart transplant (n = 1), and autopsy (n = 1). Eight of 13 (61.5 %) patients with isolated CS had a secondary prevention indication (VT in 6 and VF in 2) vs. 80 of 222 (36.0 %) with sarcoidosis in other organs (p = 0.04). Over a mean of 4.2 years, 9 of 13 (69.2 %) patients with isolated CS received appropriate ICD therapy, including anti-tachycardia pacing (ATP) and/or shock, compared with 75 of 222 (33.8 %) patients with cardiac and extracardiac sarcoidosis (p = 0.0150). Six of 7 (85.7 %) patients with definite isolated CS received appropriate ICD intervention, compared with 78 of 228 patients (34.2 %) without definite isolated CS (p = 0.0192.)
Conclusions
In this retrospective study, patients with isolated CS had very high rates of appropriate ICD therapy. Prospective, long-term follow-up of consecutive patients with isolated CS is needed to determine the true natural history and rates of ventricular arrhythmias in this rare and difficult-to-diagnose disease.


Similar content being viewed by others

Abbreviations
- ATP:
-
Anti-tachycardia pacing
- CMR:
-
Cardiac magnetic resonance
- CS:
-
Cardiac sarcoidosis
- DE:
-
Delayed enhancement
- ECG:
-
Electrocardiogram
- ICD:
-
Implantable cardiac defibrillator
- LVEF:
-
Left ventricular ejection fraction
References
Silverman, K. J., Hutchins, G. M., & Bulkley, B. H. (1978). Cardiac sarcoid: a clinicopathologic study of 84 unselected patients with systemic sarcoidosis. Circulation, 58, 1204–11.
Chinitz, J. S., Inra, L. A., Stein, K. M., & Weinsaft, J. W. (2010). Isolated cardiac sarcoid in a patient with unexplained syncope. Journal of Cardiovascular Electrophysiology, 21, 333.
Chang, T. I., Chi, N. H., Chou, N. K., Tsao, C. I., Yu, H. Y., Chen, Y. S., et al. (2012). Isolated cardiac sarcoidosis in heart transplantation. Transplantation Proceedings, 44, 903–6.
Suranagi, V. V., Malur, P. R., & Bannur, H. B. (2009). Cardiac sarcoidosis causing sudden death. Indian Journal of Pathology and Microbiology, 52, 566–7.
Kron, J., Sauer, W., Schuller, J., Bogun, F., Crawford, T., Sarsam, S., et al. (2013). Efficacy and safety of implantable cardiac defibrillators for treatment of ventricular arrhythmias in patients with cardiac sarcoidosis. Europace, 15, 347–54.
Amado, L. C., Gerber, B. L., Gupta, S. N., Rettmann, D. W., Szarf, G., Schock, R., et al. (2004). Accurate and objective infarct sizing by contrast-enhanced magnetic resonance imaging in a canine myocardial infarction model. Journal of the American College of Cardiology, 44, 2383–9.
Patel, M. R., Cawley, P. J., Heitner, J. F., Klem, I., Parker, M. A., Jaroudi, W. A., et al. (2009). Detection of myocardial damage in patients with sarcoidosis. Circulation, 120, 1969–77.
Isner, J. M., & Roberts, W. C. (1978). Right ventricular infarction complicating left ventricular infarction secondary to coronary heart disease. Frequency, location, associated findings and significance from analysis of 236 necropsy patients with acute or healed myocardial infarction. American Journal of Cardiology, 42, 885–94.
Nery, P. B., Leung, E., & Birnie, D. H. (2012). Arrhythmias in cardiac sarcoidosis: diagnosis and treatment. Current Opinion in Cardiology, 27, 181–9.
Sugizaki, Y., Tanaka, H., Imanishi, J., Konishi, A., Yamashita, T., Shinke, T., et al. (2013). Isolated primary cardiac sarcoidosis presenting as acute heart failure. Internal Medicine, 52, 71–4.
White, J., Sutton, T., & Kerr, A. (2010). Isolated primary cardiac sarcoidosis: MRI diagnosis and monitoring of treatment response with cardiac enzymes. Circulation. Heart Failure, 3, e28–9.
Brown, M. L., Reeder, G., Unni, K. K., & Mullany, C. (2007). Intraoperative diagnosis of isolated cardiac sarcoid. Heart, Lung & Circulation, 16, 315–7.
Roberts, W. C., Chung, M. S., Ko, J. M., Capehart, J. E., & Hall, S. A. (2014). Morphologic features of cardiac sarcoidosis in native hearts of patients having cardiac transplantation. American Journal of Cardiology, 113, 706–12.
Hiraga H, Yuwai K, Hiroe M, et al. (1993). Guideline for diagnosis of cardiac sarcoidosis: study report on diffuse pulmonary diseases from the Japanese Ministry of Health and Welfare. Tokyo: Japanese Ministry of Health and Welfare. 23–4 (in Japanese).
Ardehali, H., Howard, D. L., Hariri, A., Qasim, A., Hare, J. M., Baughman, K. L., et al. (2005). A positive endomyocardial biopsy result for sarcoid is associated with poor prognosis in patients with initially unexplained cardiomyopathy. American Heart Journal, 150, 459–63.
(2007).Diagnostic standard and guidelines for sarcoidosis. Jpn J Sarcoidosis Granulomatous Disord.; 27: 89–102 (in Japanese).
Birnie, D. H., Sauer, W. H., Bogun, F., Cooper, J. M., Culver, D. A., Duvernoy, C. S., et al. (2014). HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm, 11, 1305–23.
Nery, P. B., Keren, A., Healey, J., Leug, E., Beanlands, R. S., & Birnie, D. H. (2013). Isolated cardiac sarcoidosis: establishing the diagnosis with electroanatomic mapping-guided endomyocardial biopsy. Canadian Journal of Cardiology, 29, 1015.e1–3.
Smedema, J. P., Snoep, G., van Kroonenburgh, M. P., van Geuns, R. J., Dassen, W. R., Gorgels, A. P., et al. (2005). Evaluation of the accuracy of gadolinium-enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. Journal of the American College of Cardiology, 45, 1683–90.
Nelson, J. E., Kirschner, P. A., & Teirstein, A. S. (1996). Sarcoidosis presenting as heart disease. Sarcoidosis, Vasculitis, and Diffuse Lung Diseases, 13, 178–82.
Conflict of interest
Dr. Kron has reported that she has no relationships relevant to the contents of this paper to disclose.
Dr. Sauer has reported that he received education grants for EP fellowship and consulting fees from Medtronic Inc., St. Jude Medical, and Boston Scientific Corp.
Dr. Mueller has reported that she has no relationship relevant to the contents of this paper to disclose.
Dr. Schuller has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Bogun has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Sarsam has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Rosenfeld has reported that she has received fellowship support from Medtronic Inc., Boston Scientific, and St. Jude Medical.
Dr. Mitiku has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Cooper has received honoraria from Medtronic Inc., Boston Scientific, Biotronik, St. Jude Medical, and Spectranetics.
Dr. Mehta has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Greenspon has received honoraria from Medtronic Inc., Boston Scientific, and St. Jude Medical.
Dr. Ortman has received speaking fees from St. Jude Medical and Boston Scientific.
Dr. Delurgio has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Valadri has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Narasimhan has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Swapna has reported that she has no relationships relevant to the contents of this paper to disclose.
Dr. Singh has reported that he received research grants from St. Jude Medical, Medtronic Inc., Boston Scientific Corp., and Biotronik; consultant fees from Boston Scientific Corp., Biotronik, St. Jude Medical, Medtronic Inc., CardioInsight Inc., Thoratec Inc., and Biosense Webster; honoraria from Medtronic Inc., Biotronik, Guidant Corp., St. Jude Medical, and Sorin Group.
Dr. Danik has reported consultant fees from St. Jude Medical, Boston Scientific.
Dr. Markowitz has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Almquist has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Krahn has reported that he has no relationships relevant to the contents of this paper to disclose.
Mr. Wolfe has reported that he has no relationships relevant to the contents of this paper to disclose.
Mr. Feinstein has reported that he has no relationships relevant to the contents of this paper to disclose.
Dr. Ellenbogen has received honoraria from Medtronic Inc., Boston Scientific, and Cameron Medical; speaking fees from Medtronic Inc., Boston Scientific, St. Jude Medical, Biotronik, and Sanofi; research grants from Medtronic Inc., Boston Scientific, Biosense Web, and Sanofi; fellowship support from Medtronic Inc., Boston Scientific, and Biosense Web.
Dr. Crawford has received grant support from Cardiovascular Center at the University of Michigan and Boston Scientific, Inc. for the development and maintenance of cardiac sarcoidosis registry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kron, J., Sauer, W., Mueller, G. et al. Outcomes of patients with definite and suspected isolated cardiac sarcoidosis treated with an implantable cardiac defibrillator. J Interv Card Electrophysiol 43, 55–64 (2015). https://doi.org/10.1007/s10840-015-9978-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-015-9978-3