
Assessment of PI3K/mTOR/AKT Pathway Elements to Serve as Biomarkers and Therapeutic Targets in Penile Cancer

 , , , ,
, , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Immunohistochemical Staining
2.3. p16INK4a Staining
2.4. Staining Evaluation
2.5. HPV DNA Detection
2.6. Cell Culture
2.7. Therapeutic Agent
2.8. Measurement of Cell Viability
2.9. Chemotatic Activity of PeCa Cell Lines
2.10. Western Blot
2.11. Statistical Analysis
3. Results
3.1. Clinicopathological Data
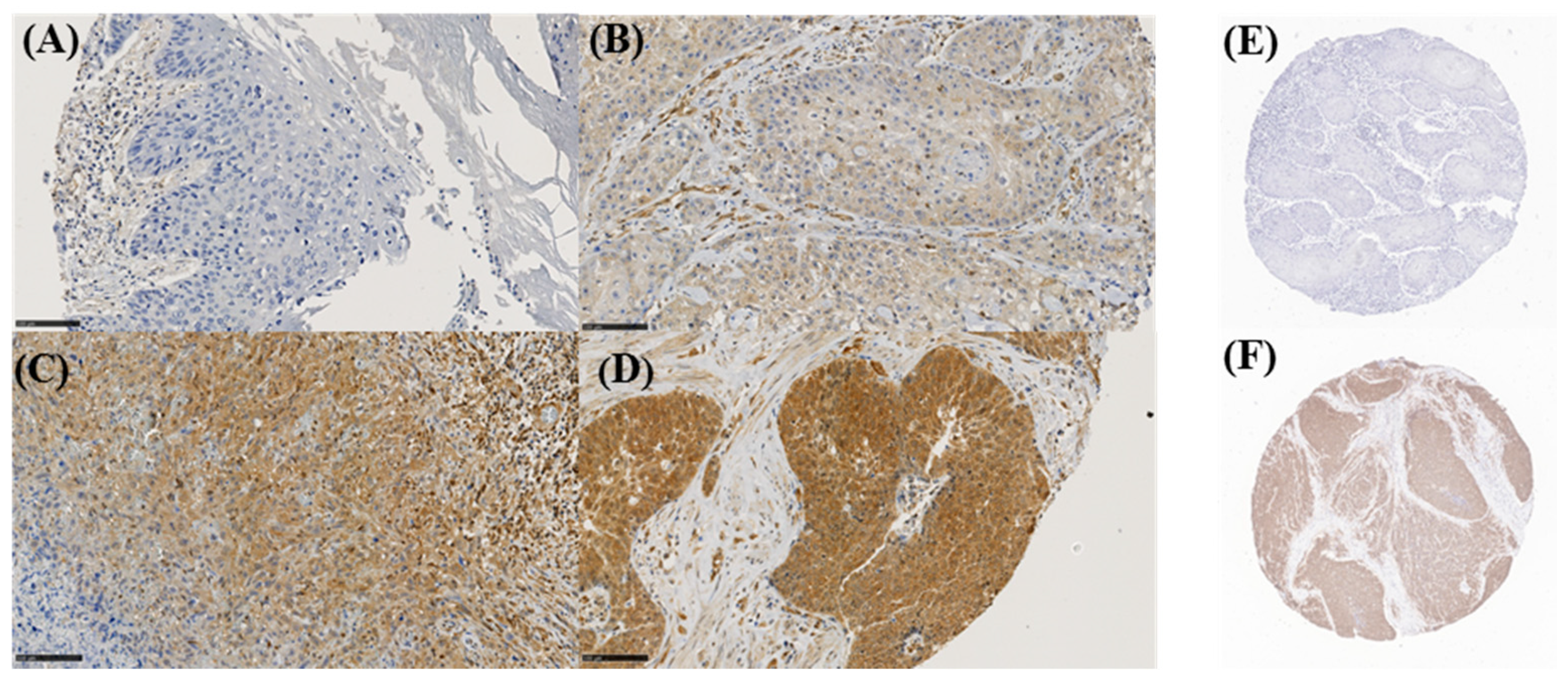
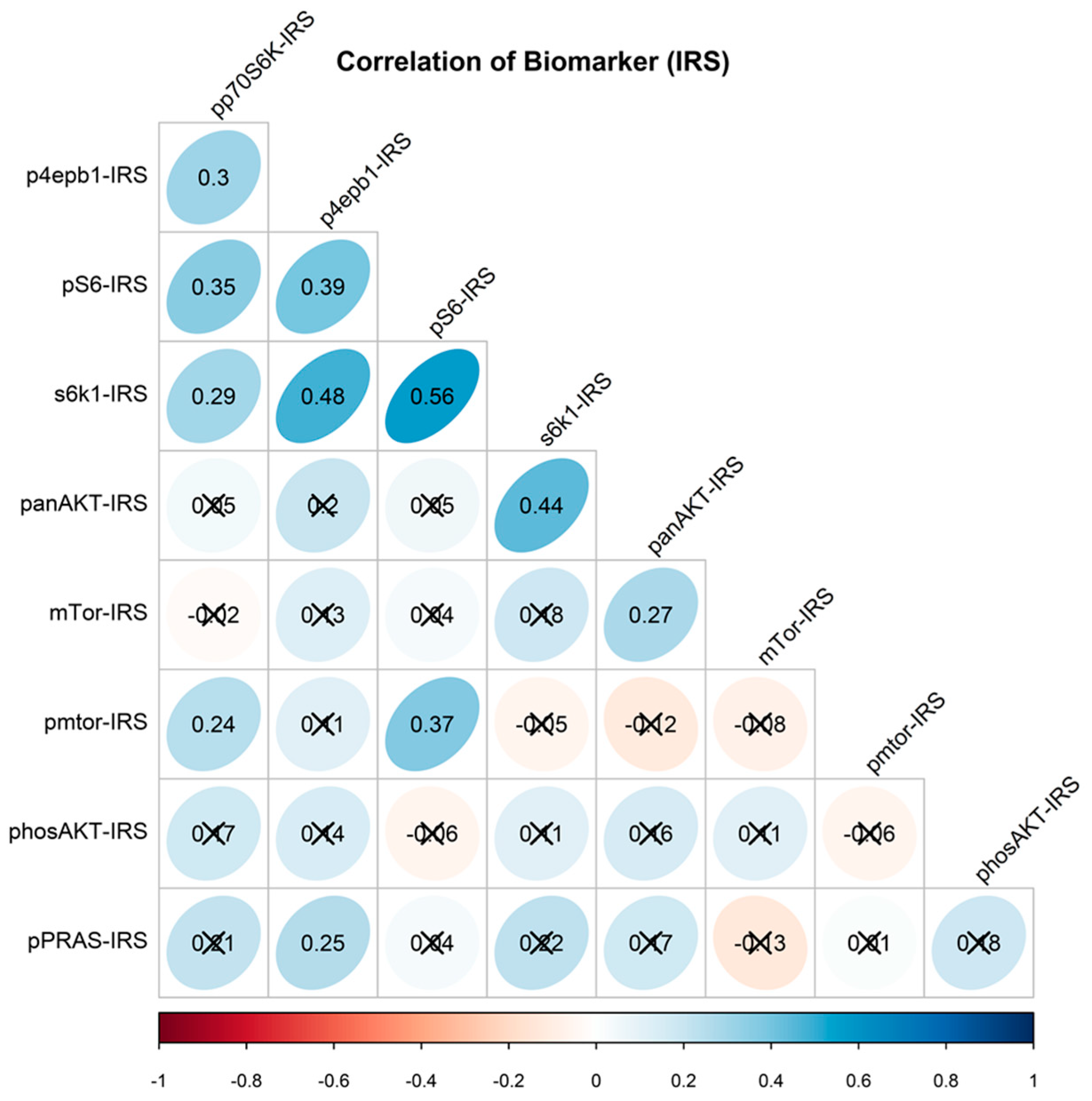
3.2. Tumor Marker Expression and Associations
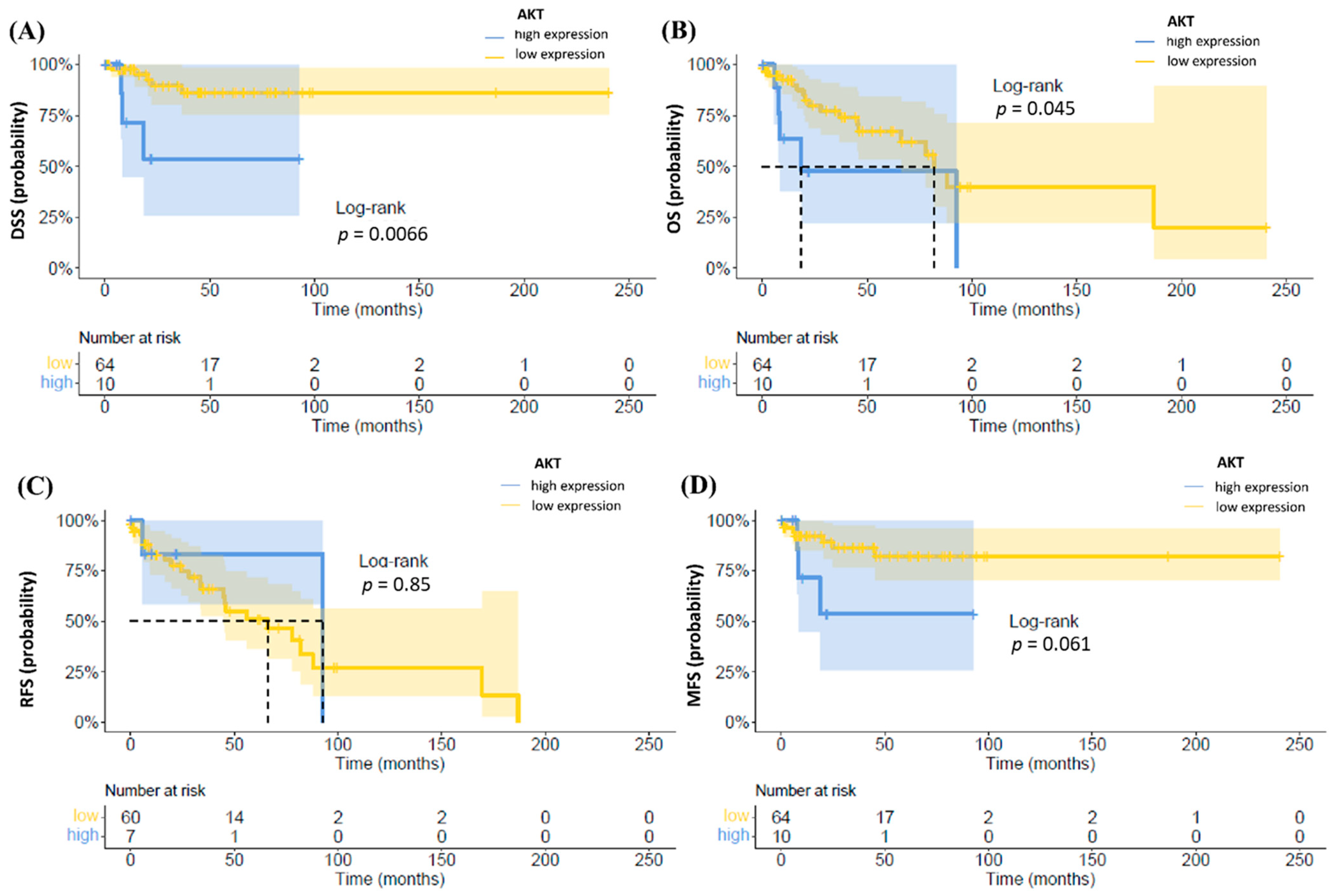
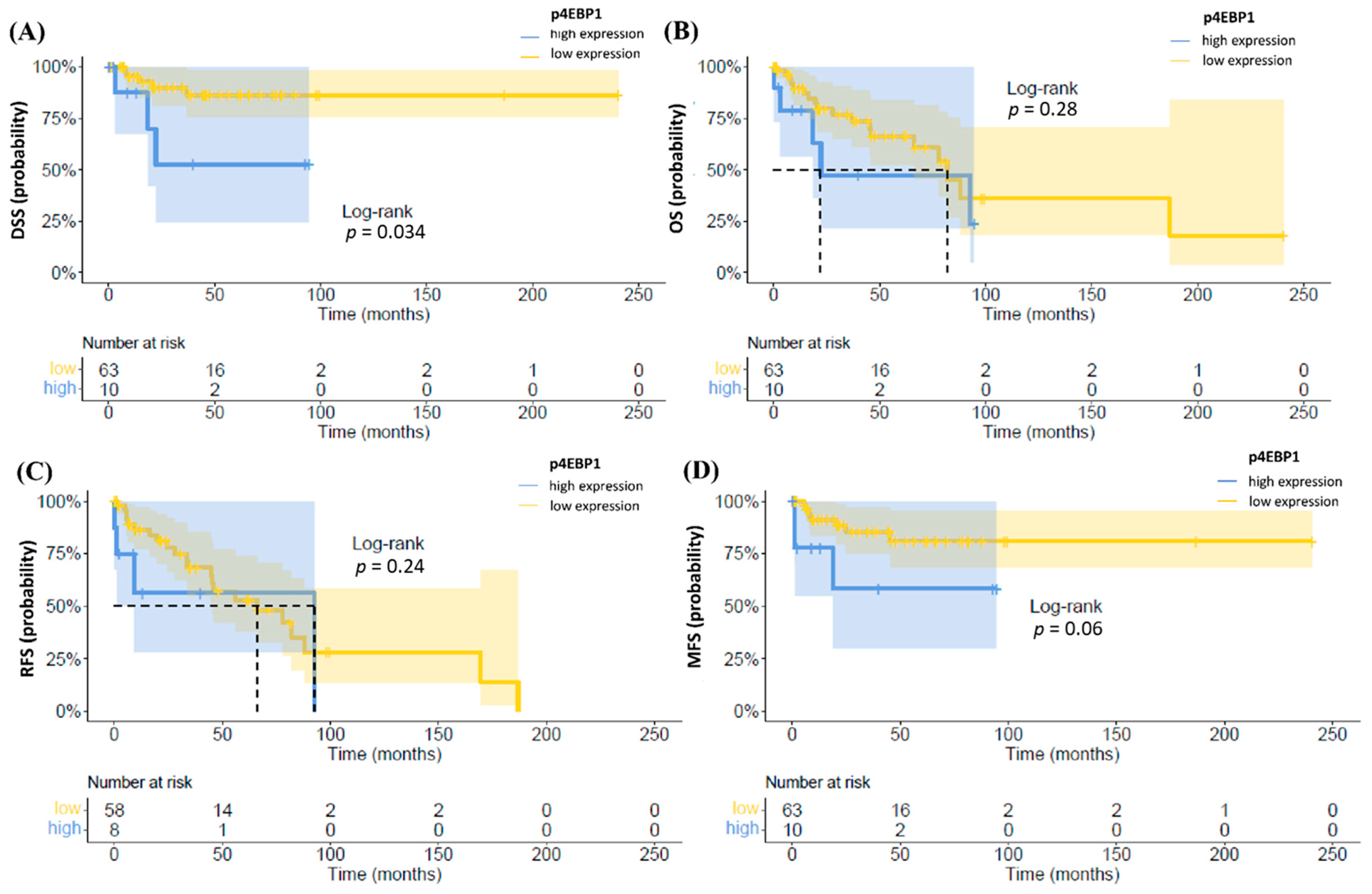
3.3. Follow-Up and Survival
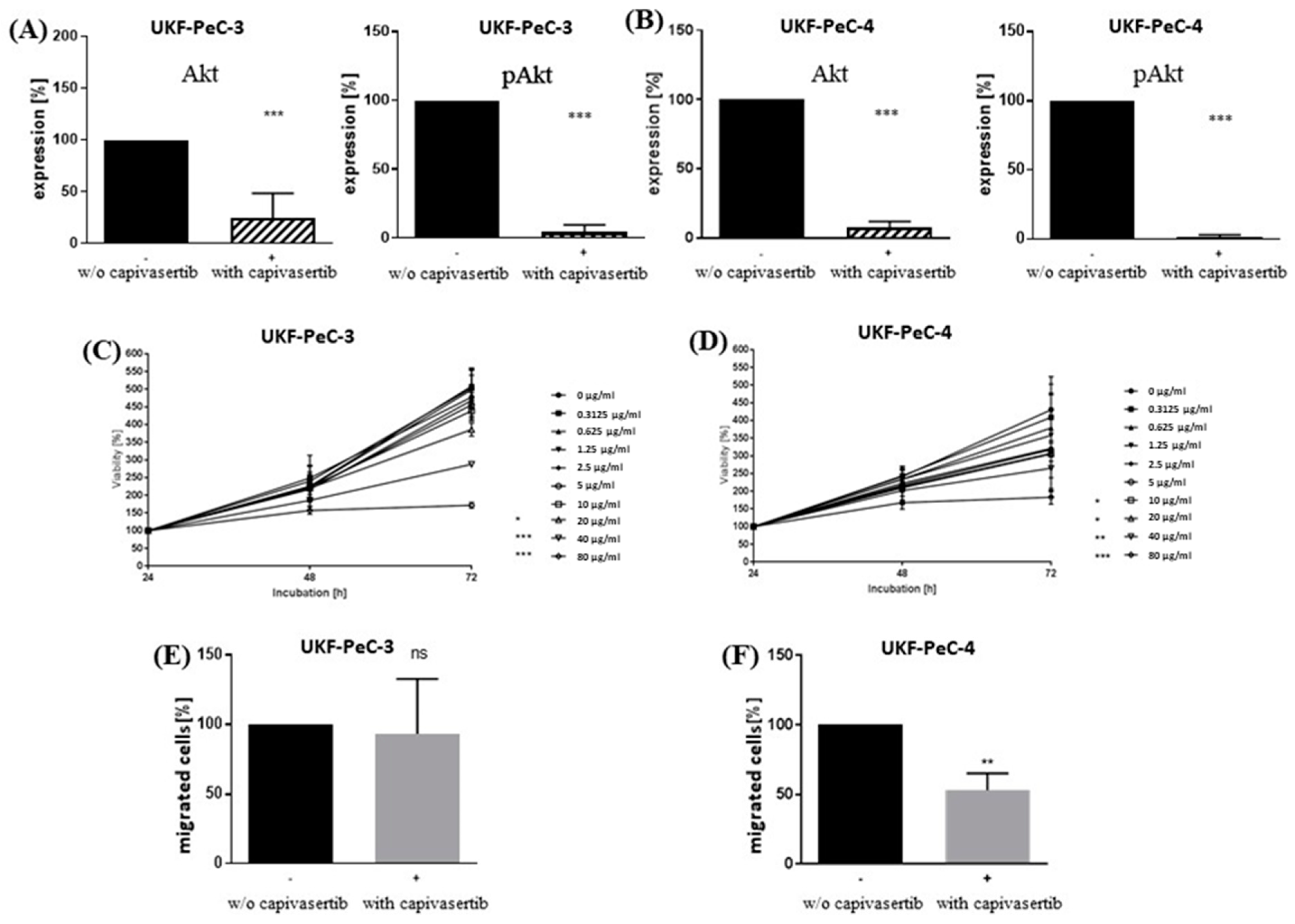
3.4. Impact of AKT Blockade on Tumor Cell Growth
3.5. Modulation of Motility by AKT Inhibition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hakenberg, O.W.; Compérat, E.M.; Minhas, S.; Necchi, A.; Protzel, C.; Watkin, N. EAU Guidelines on Penile Cancer: 2014 Update. Eur. Urol. 2015, 67, 142–150. [Google Scholar] [CrossRef]
- Thomas, A.; Necchi, A.; Muneer, A.; Tobias-Machado, M.; Tran, A.T.H.; Van Rompuy, A.-S.; Spiess, P.E.; Albersen, M. Penile cancer. Nat. Rev. Dis. Prim. 2021, 7, 1–24. [Google Scholar] [CrossRef]
- Wang, J.; Pettaway, C.A.; Pagliaro, L.C. Treatment for Metastatic Penile Cancer After First-line Chemotherapy Failure: Analysis of Response and Survival Outcomes. Urology 2015, 85, 1104–1110. [Google Scholar] [CrossRef]
- Sun, H.; Lesche, R.; Li, D.-M.; Liliental, J.; Zhang, H.; Gao, J.; Gavrilova, N.; Mueller, B.; Liu, X.; Wu, H. PTEN modulates cell cycle progression and cell survival by regulating phosphatidylinositol 3,4,5,-trisphosphate and Akt/protein kinase B signaling pathway. Proc. Natl. Acad. Sci. USA 1999, 96, 6199–6204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LoPiccolo, J.; Blumenthal, G.M.; Bernstein, W.B.; Dennis, P.A. Targeting the PI3K/Akt/mTOR pathway: Effective combinations and clinical considerations. Drug Resist. Updat. 2008, 11, 32–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, K.; Stokoe, D.; Taketani, Y.; McCormick, F. High Frequency of Coexistent Mutations of PIK3CA and PTEN Genes in Endometrial Carcinoma. Cancer Res. 2005, 65, 10669–10673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, Y.; Wang, Z.; Bardelli, A.; Silliman, N.; Ptak, J.; Szabo, S.; Yan, H.; Gazdar, A.; Powell, S.M.; Riggins, G.J.; et al. High Frequency of Mutations of the PIK3CA Gene in Human Cancers. Science 2004, 304, 554. [Google Scholar] [CrossRef] [Green Version]
- Page, C.; Huang, M.; Jin, X.; Cho, K.; Lilja, J.; Reynolds, R.K.; Lin, J. Elevated phosphorylation of AKT and Stat3 in prostate, breast, and cervical cancer cells. Int. J. Oncol. 2000, 17, 23–31. [Google Scholar] [CrossRef]
- Campbell, I.G.; Russell, S.E.; Choong, D.Y.H.; Montgomery, K.G.; Ciavarella, M.L.; Hooi, C.S.F.; Cristiano, B.E.; Pearson, R.B.; Phillips, W.A. Mutation of the PIK3CA Gene in Ovarian and Breast Cancer. Cancer Res. 2004, 64, 7678–7681. [Google Scholar] [CrossRef] [Green Version]
- Ligresti, G.; Militello, L.; Steelman, L.S.; Cavallaro, A.; Basile, F.; Nicoletti, F.; Stivala, F.; McCubrey, J.A.; Libra, M. PIK3CA mutations in human solid tumors: Role in sensitivity to various therapeutic approaches. Cell Cycle 2009, 8, 1352–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stahl, J.M.; Sharma, A.; Cheung, M.; Zimmerman, M.; Cheng, J.Q.; Bosenberg, M.W.; Kester, M.; Sandirasegarane, L.; Robertson, G.P. Deregulated Akt3 Activity Promotes Development of Malignant Melanoma. Cancer Res. 2004, 64, 7002–7010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicenas, J. The potential role of Akt phosphorylation in human cancers. Int. J. Biol. Markers 2008, 23. [Google Scholar] [CrossRef]
- Leijte, J.A.; Kirrander, P.; Antonini, N.; Windahl, T.; Horenblas, S. Recurrence Patterns of Squamous Cell Carcinoma of the Penis: Recommendations for Follow-Up Based on a Two-Centre Analysis of 700 Patients. Eur. Urol. 2008, 54, 161–169. [Google Scholar] [CrossRef]
- Macher-Goeppinger, S.; Aulmann, S.; Tagscherer, K.E.; Wagener, N.; Haferkamp, A.; Penzel, R.; Brauckhoff, A.; Hohenfellner, M.; Sykora, J.; Walczak, H.; et al. Prognostic Value of Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAIL) and TRAIL Receptors in Renal Cell Cancer. Clin. Cancer Res. 2009, 15, 650–659. [Google Scholar] [CrossRef] [Green Version]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Der Pathol. 1987, 8, 138–140. [Google Scholar]
- Hoo, Z.H.; Candlish, J.; Teare, D. What is an ROC curve? Emerg. Med. J. 2017, 34, 357–359. [Google Scholar] [CrossRef] [PubMed]
- Kotchetkov, R.; Cinatl, J.; Blaheta, R.; Vogel, J.-U.; Karaskova, J.; Squire, J.; Driever, P.H.; Klingebiel, T.; Cinatl, J., Jr. Development of resistance to vincristine and doxorubicin in neuroblastoma alters malignant properties and induces additional karyotype changes: A preclinical model. Int. J. Cancer 2002, 104, 36–43. [Google Scholar] [CrossRef]
- Kotchetkov, R.; Driever, P.H.; Cinatl, J.; Michaelis, M.; Karaskova, J.; Blaheta, R.; Squire, J.A.; Von Deimling, A.; Moog, J.; Cinatl, J. Increased malignant behavior in neuroblastoma cells with acquired multi-drug resistance does not depend on P-gp expression. Int. J. Oncol. 2005, 27, 1029–1037. [Google Scholar] [CrossRef]
- Robertson, J.F.; Coleman, R.E.; Cheung, K.-L.; Evans, A.; Holcombe, C.; Skene, A.; Rea, D.; Ahmed, S.; Jahan, A.; Horgan, K.; et al. Proliferation and AKT Activity Biomarker Analyses after Capivasertib (AZD5363) Treatment of Patients with ER+ Invasive Breast Cancer (STAKT). Clin. Cancer Res. 2020, 26, 1574–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolinsky, M.; Rescigno, P.; Bianchini, D.; Zafeiriou, Z.; Mehra, N.; Mateo, J.; Michalarea, V.; Riisnaes, R.; Crespo, M.; Figueiredo, I.; et al. A phase I dose-escalation study of enzalutamide in combination with the AKT inhibitor AZD5363 (capivasertib) in patients with metastatic castration-resistant prostate cancer. Ann. Oncol. 2020, 31, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Thomas, A.; do Canto Alvim, L.M.; Rainho, C.A.; Juengel, E.; Blaheta, R.A.; Spiess, P.E.; Rogatto, S.R.; Tsaur, I. Urology. In Systemic Treatment of Penile Squamous Cell Carcinoma—Hurdles and Hopes of Preclinical Models and Clinical Regimens: A Narrative Review. Transl. Androl. Urol. 2020. [Google Scholar] [CrossRef]
- Ferrándiz-Pulido, C.; Hernández-Losa, J.; Masferrer, E.; Vivancos, A.; Somoza, R.; Mares, R.; Valverde, C.; Salvador, C.; Placer, J.; Morote, J.; et al. Identification of somatic gene mutations in penile squamous cell carcinoma. Genes Chromosom. Cancer 2015, 54, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.S. PI3K/Akt/mTOR inhibitors in cancer: At the bench and bedside. Semin. Cancer Biol. 2019, 59, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Popova, N.V.; Jücker, M. The Role of mTOR Signaling as a Therapeutic Target in Cancer. Int. J. Mol. Sci. 2021, 22, 1743. [Google Scholar] [CrossRef]
- Azizi, M.; Tang, D.H.; Verduzco, D.; Peyton, C.C.; Chipollini, J.; Yuan, Z.; Schaible, B.J.; Zhou, J.M.; Johnstone, P.A.; Giuliano, A.; et al. Impact of PI3K-AKT-mTOR Signaling Pathway Up-regulation on Prognosis of Penile Squamous-Cell Carcinoma: Results from a Tissue Microarray Study and Review of the Literature. Clin. Genitourin. Cancer 2019, 17, e80–e91. [Google Scholar] [CrossRef]
- Chaux, A.; Munari, E.; Cubilla, A.L.; Hicks, J.; Lecksell, K.; Burnett, A.L.; Netto, G.J. Immunohistochemical expression of the mammalian target of rapamycin pathway in penile squamous cell carcinomas: A tissue microarray study of 112 cases. Histopathology 2014, 64, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, F.S.; Andrade, M.F.; Loyola, A.M.; da Silva, S.J.; Silva, M.J.B.; Cardoso, S.V.; de Faria, P.R. Pathologic significance of AKT, mTOR, and GSK3beta proteins in oral squamous cell carcinoma-affected patients. Virchows Arch. 2018, 472, 983–997. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.M.; Yu, J.; Khoury, T.; Chadha, K.C.; Iyer, R.V.; Foster, J.; Kuvshinoff, B.W.; Gibbs, J.F.; Geradts, J.; Black, J.D.; et al. Akt expression may predict favorable prognosis in cholangiocarcinoma. J. Gastroenterol. Hepatol. 2006, 21, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Lindner, A.K.; Schachtner, G.; Steiner, E.; Kroiss, A.; Uprimny, C.; Steinkohl, F.; Horninger, W.; Heidegger, I.; Madersbacher, S.; Pichler, R. Organ-sparing surgery of penile cancer: Higher rate of local recurrence yet no impact on overall survival. World J. Urol. 2020, 38, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Kreisberg, J.I.; Malik, S.N.; Prihoda, T.J.; Bedolla, R.G.; Troyer, D.A.; Kreisberg, S.; Ghosh, P.M. Phosphorylation of Akt (Ser473) is an Excellent Predictor of Poor Clinical Outcome in Prostate Cancer. Cancer Res. 2004, 64, 5232–5236. [Google Scholar] [CrossRef] [Green Version]
- Dai, D.L.; Martinka, M.; Li, G. Prognostic Significance of Activated Akt Expression in Melanoma: A Clinicopathologic Study of 292 Cases. J. Clin. Oncol. 2005, 23, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zang, H.; Zheng, H.; Zhan, Y.; Yang, Y.; Zhang, Y.; Liu, S.; Feng, J.; Wen, Q.; Long, M.; et al. Overexpression of p-Akt, p-mTOR and p-eIF4E proteins associates with metastasis and unfavorable prognosis in non-small cell lung cancer. PLoS ONE 2020, 15, e0227768. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.; Swain, W.A.; Richardson, D.; Edwards, J.; Stewart, D.J.; Richardson, C.M.; Swinson, D.E.B.; Patel, D.; Jones, J.L.; O’Byrne, K.J. Phospho-Akt Expression Is Associated with a Favorable Outcome in Non–Small Cell Lung Cancer. Clin. Cancer Res. 2005, 11, 2930–2936. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.-Z.; Zhou, X.-D.; Qian, G.; Shi, X.; Fang, J.; Jiang, B.-H. AKT1 Amplification Regulates Cisplatin Resistance in Human Lung Cancer Cells through the Mammalian Target of Rapamycin/p70S6K1 Pathway. Cancer Res. 2007, 67, 6325–6332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhang, L.-L.; Shen, L.; Xu, X.-M.; Yu, H.-G. Regulation of AKT gene expression by cisplatin. Oncol. Lett. 2013, 5, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.R.; Greenwood, H.; Dudley, P.; Crafter, C.; Yu, D.-H.; Zhang, J.; Li, J.; Gao, B.; Ji, Q.; Maynard, J.; et al. Preclinical Pharmacology of AZD5363, an Inhibitor of AKT: Pharmacodynamics, Antitumor Activity, and Correlation of Monotherapy Activity with Genetic Background. Mol. Cancer Ther. 2012, 11, 873–887. [Google Scholar] [CrossRef] [Green Version]
- Davies, B.R.; Guan, N.; Logie, A.; Crafter, C.; Hanson, L.; Jacobs, V.; James, N.H.; Dudley, P.; Jacques, K.; Ladd, B.; et al. Tumors with AKT1E17K Mutations Are Rational Targets for Single Agent or Combination Therapy with AKT Inhibitors. Mol. Cancer Ther. 2015, 14, 2441–2451. [Google Scholar] [CrossRef] [Green Version]
- Stankiewicz, E.; Prowse, D.M.; Ng, M.; Cuzick, J.; Mesher, D.; Hiscock, F.; Lu, Y.-J.; Watkin, N.; Corbishley, C.; Lam, W.; et al. Alternative HER/PTEN/Akt Pathway Activation in HPV Positive and Negative Penile Carcinomas. PLoS ONE 2011, 6, e17517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J. Signaling pathways in HPV-associated cancers and therapeutic implications. Rev. Med. Virol. 2015, 25, 24–53. [Google Scholar] [CrossRef]
- Kalinsky, K.; Hong, F.; McCourt, C.K.; Sachdev, J.C.; Mitchell, E.P.; Zwiebel, J.A.; Doyle, L.A.; McShane, L.M.; Li, S.; Gray, R.J.; et al. Effect of Capivasertib in Patients with an AKT1 E17K-Mutated Tumor: NCI-MATCH Subprotocol EAY131-Y Nonrandomized Trial. JAMA Oncol. 2021, 7, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Stemke-Hale, K.; Gonzalez-Angulo, A.M.; Lluch, A.; Neve, R.M.; Kuo, W.-L.; Davies, M.; Carey, M.; Yinghui, G.; Guan, Y.; Sahin, A.; et al. An Integrative Genomic and Proteomic Analysis of PIK3CA, PTEN, and AKT Mutations in Breast Cancer. Cancer Res. 2008, 68, 6084–6091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Abraham, J.; Chan, S.; Wheatley, D.; Brunt, A.M.; Nemsadze, G.; Baird, R.D.; Park, Y.H.; Hall, P.S.; Perren, T.; et al. Capivasertib Plus Paclitaxel Versus Placebo Plus Paclitaxel as First-Line Therapy for Metastatic Triple-Negative Breast Cancer: The PAKT Trial. J. Clin. Oncol. 2020, 38, 423–433. [Google Scholar] [CrossRef]
- Wu, Y.-H.; Huang, Y.-F.; Chen, C.-C.; Huang, C.-Y.; Chou, C.-Y. Comparing PI3K/Akt Inhibitors Used in Ovarian Cancer Treatment. Front. Pharmacol. 2020, 11, 206. [Google Scholar] [CrossRef] [Green Version]
- Ferrandiz-Pulido, C.; Masferrer, E.; Toll, A.; Hernandez-Losa, J.; Mojal, S.; Pujol, R.M.; Cajal, S.R.Y.; De Torres, I.; Garcia-Patos, V. mTOR Signaling Pathway in Penile Squamous Cell Carcinoma: pmTOR and peIF4E Over Expression Correlate with Aggressive Tumor Behavior. J. Urol. 2013, 190, 2288–2295. [Google Scholar] [CrossRef]
- Wen, S.; Ren, W.; Xue, B.; Fan, Y.; Jiang, Y.; Zeng, C.; Li, Y.; Zu, X. Prognostic factors in patients with penile cancer after surgical management. World J. Urol. 2018, 36, 435–440. [Google Scholar] [CrossRef]
- Li, Z.-S.; Yao, K.; Chen, P.; Zou, Z.-J.; Qin, Z.-K.; Liu, Z.-W.; Li, Y.-H.; Zhou, F.-J.; Han, H. Disease-specific survival after radical lymphadenectomy for penile cancer: Prediction by lymph node count and density11This work was supported by the Science and Technology Foundation of the Guangdong Province (2012B031800079 to H. Han).2Zai-shang Li and Kai Yao contributed equally to this article. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 893–900. [Google Scholar] [CrossRef]
- Emerson, R.E.; Ulbright, T.M.; Eble, J.N.; Geary, W.A.; Eckert, G.J.; Cheng, L. Predicting Cancer Progression in Patients with Penile Squamous Cell Carcinoma: The Importance of Depth of Invasion and Vascular Invasion. Mod. Pathol. 2001, 14, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.-C.; Fizazi, K.; Piron, D.; Kramar, A.; Gerbaulet, A.; Haie-Meder, C.; Perrin, J.-L.; Court, B.; Wibault, P.; Théodore, C. Squamous cell carcinoma of the penis: Multivariate analysis of prognostic factors and natural history in a monocentric study with a conservative policy. Ann. Oncol. 1997, 8, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Evren, S.; Dermen, A.; Lockwood, G.; Fleshner, N.; Sweet, J. Immunohistochemical examination of the mTORC1 pathway in high grade prostatic intraepithelial neoplasia (HGPIN) and prostatic adenocarcinomas (PCa): A tissue microarray study (TMA). Prostate 2010, 70, 1429–1436. [Google Scholar] [CrossRef]
- Brugarolas, J.; Lei, K.; Hurley, R.L.; Manning, B.D.; Reiling, J.H.; Hafen, E.; Witters, L.A.; Ellisen, L.W.; Kaelin, W.G. Regulation of mTOR function in response to hypoxia by REDD1 and the TSC1/TSC2 tumor suppressor complex. Genes Dev. 2004, 18, 2893–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Wang, Z.; Huang, J.; Cheng, S.; Du, H.; Che, G.; Peng, Y. Clinicopathological and prognostic significance of mTOR and phosphorylated mTOR expression in patients with esophageal squamous cell carcinoma: A systematic review and meta-analysis. BMC Cancer 2016, 16, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Zoncu, R.; Efeyan, A.; Sabatini, D.M. mTOR: From growth signal integration to cancer, diabetes and ageing. Nat. Rev. Mol. Cell Biol. 2010, 12, 21–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, B.R.; Mossanen, M.; Holt, S.K.; Lin, D.W.; Wright, J.L. Predictors of Nodal Upstaging in Clinical Node Negative Patients with Penile Carcinoma: A National Cancer Database Analysis. Urology 2016, 96, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Steinestel, J.; Al Ghazal, A.; Arndt, A.; Schnoeller, T.J.; Schrader, A.J.; Moeller, P.; Steinestel, K. The role of histologic subtype, p16(INK4a) expression, and presence of human papillomavirus DNA in penile squamous cell carcinoma. BMC Cancer 2015, 15, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Overall (n = 76) |
|---|---|
| Age at diagnosis | |
| Mean (SD) | 64.1 (11.9) |
| Median [Min, Max] | 67.0 [31.0, 86.0] |
| ≤65 | 36 (47.4%) |
| >65 | 40 (52.6%) |
| Primary tumor surgery | |
| Circumcision | 8 (10.5%) |
| Tumor excision | 3 (3.9%) |
| Partial penectomy | 44 (57.9%) |
| Total penectomy | 21 (27.6%) |
| Primary tumor grade | |
| Low (G1/G2) | 59 (77.6%) |
| High (G3/G4) | 17 (22.4%) |
| Pathologic T stage | |
| pT1 | 32 (42.1%) |
| pT2 | 26 (34.2%) |
| pT3 | 18 (23.7%) |
| Pathologic T1 subtypes | |
| pT1a | 7 (21,9%) |
| pT1b | 2 (6,2%) |
| Missing | 23 (71,9%) |
| Lymphovascular invasion | |
| No | 31 (40.8%) |
| Yes | 18 (23.7%) |
| Missing | 27 (35.5%) |
| HPV infection | |
| Negative | 56 (73.7%) |
| Positive | 18 (23.7%) |
| Missing | 2 (2.6%) |
| p16INK4a status | |
| Negative | 35 (46.1%) |
| Positive | 38 (50.0%) |
| Missing | 3 (3.9%) |
| Pathologic N stage | |
| NX-0 | 62 (81.6%) |
| N1 | 4 (5.3%) |
| N2 | 7 (9.2%) |
| N3 | 3 (3.9%) |
| Recurrence status | |
| No | 58 (76.3%) |
| Yes | 18 (23.7%) |
| Recurrence location | |
| None | 58 (76.3%) |
| Local | 8 (10.5%) |
| Regional | 1 (1.3%) |
| Distant | 9 (11.8%) |
| Subsequent therapy | |
| None | 60 (78.9%) |
| CTX | 13 (17.1%) |
| Radiation | 1 (1.3%) |
| CTX and Radiation | 2 (2.6%) |
| Tumor-dependent death | |
| No | 68 (89.5%) |
| Yes | 8 (10.5%) |
| Characteristic | OS | DSS | RFS | MFS | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Age at diagnosis ≤65 >65 Lymph node metastasis | 1.00 (reference) 3.07 (0.72–13.02) | 0.128 | ||||||
| Negative | 1.00 (reference) | 1.00 (reference) | ||||||
| Positive | 36 (3.33–391) | 0.003 | 11.97 (2.70–53.12) | 0.001 | ||||
| Primary tumor | ||||||||
| pT1 | 1.00 (reference) | |||||||
| pT2/pT3 | 0.318 (0.09–1.16) | 0.0837 | ||||||
| Diabetes | ||||||||
| Negative | 1.00 (reference) | |||||||
| Positive | 3.86 (1.07–13.86) | 0.0384 | ||||||
| HTN | ||||||||
| Negative | 1.00 (reference) | |||||||
| Positive | 0.337 (0.09–1.23) | 0.0987 | ||||||
| COPD | ||||||||
| Negative | 1.00 (reference) | |||||||
| Positive | 2.86 (0.73–11.27) | 0.133 | ||||||
| Phimose | ||||||||
| Negative | 1.00 (reference) | |||||||
| Positive | 0.246 (0.07–0.89) | 0.0333 | ||||||
| TNM N stage | ||||||||
| Negative | 1.00 (reference) | |||||||
| Positive | 0.287 (0.05–1.67) | 0.164 | ||||||
| Grading | ||||||||
| G1/G2 | 0.43 (0.16–1.18) | 0.102 | ||||||
| G3/G4 | 1.00 (reference) | |||||||
| AKT | ||||||||
| Low expression | 1.00 (reference) | 1.00 (reference) | ||||||
| High expression | 3.43 (1.22–9.68) | 0.0197 | 7.53 (1.12–50.5) | 0.0377 | ||||
| pmTOR | ||||||||
| Low expression | 1.00 (reference) | |||||||
| High expression | 9.95 (1.25–79.3) | 0.0301 | ||||||
| p4epb1 | ||||||||
| Low expression | 1.00 (reference) | |||||||
| High expression | 5.99 (0.779–46.1) | 0.0855 | ||||||
| pPRAS | ||||||||
| Low expression | 1.00 (reference) | |||||||
| High expression | 0.132 (0.01–1.62) | 0.113 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, A.; Reetz, S.; Stenzel, P.; Tagscherer, K.; Roth, W.; Schindeldecker, M.; Michaelis, M.; Rothweiler, F.; Cinatl, J., Jr.; Cinatl, J.; et al. Assessment of PI3K/mTOR/AKT Pathway Elements to Serve as Biomarkers and Therapeutic Targets in Penile Cancer. Cancers 2021, 13, 2323. https://doi.org/10.3390/cancers13102323
Thomas A, Reetz S, Stenzel P, Tagscherer K, Roth W, Schindeldecker M, Michaelis M, Rothweiler F, Cinatl J Jr., Cinatl J, et al. Assessment of PI3K/mTOR/AKT Pathway Elements to Serve as Biomarkers and Therapeutic Targets in Penile Cancer. Cancers. 2021; 13(10):2323. https://doi.org/10.3390/cancers13102323
Chicago/Turabian StyleThomas, Anita, Sascha Reetz, Philipp Stenzel, Katrin Tagscherer, Wilfried Roth, Mario Schindeldecker, Martin Michaelis, Florian Rothweiler, Jindrich Cinatl, Jr., Jaroslav Cinatl, and et al. 2021. "Assessment of PI3K/mTOR/AKT Pathway Elements to Serve as Biomarkers and Therapeutic Targets in Penile Cancer" Cancers 13, no. 10: 2323. https://doi.org/10.3390/cancers13102323