Early Identification of Acute Traumatic Coagulopathy Using Clinical Prediction Tools: A Systematic Review


1
School of Public Health and Preventive Medicine, Monash University, Melbourne 3004, Australia
2
Institute for Research in Operative Medicine, University Witten/Herdecke, 51109 Cologne, Germany
3
Department of Traumatology, Orthopaedic Surgery and Sports Traumatology, Cologne-Merheim Medical Centre, 51109 Cologne, Germany
4
ANU Medical School, Australian National University, Canberra 2605, Australia
5
National Trauma Research Institute, Melbourne 3004, Australia
6
Emergency and Trauma Centre, The Alfred Hospital, Melbourne 3004, Australia
*
Author to whom correspondence should be addressed.
Medicina 2019, 55(10), 653; https://doi.org/10.3390/medicina55100653
Submission received: 8 June 2019
/
Revised: 20 September 2019
/
Accepted: 25 September 2019
/
Published: 28 September 2019
(This article belongs to the Special Issue Trauma care)
Abstract
:Background and objectives: Prompt identification of patients with acute traumatic coagulopathy (ATC) is necessary to expedite appropriate treatment. An early clinical prediction tool that does not require laboratory testing is a convenient way to estimate risk. Prediction models have been developed, but none are in widespread use. This systematic review aimed to identify and assess accuracy of prediction tools for ATC. Materials and Methods: A search of OVID Medline and Embase was performed for articles published between January 1998 and February 2018. We searched for prognostic and predictive studies of coagulopathy in adult trauma patients. Studies that described stand-alone predictive or associated factors were excluded. Studies describing prediction of laboratory-diagnosed ATC were extracted. Performance of these tools was described. Results: Six studies were identified describing four different ATC prediction tools. The COAST score uses five prehospital variables (blood pressure, temperature, chest decompression, vehicular entrapment and abdominal injury) and performed with 60% sensitivity and 96% specificity to identify an International Normalised Ratio (INR) of >1.5 on an Australian single centre cohort. TICCS predicted an INR of >1.3 in a small Belgian cohort with 100% sensitivity and 96% specificity based on admissions to resuscitation rooms, blood pressure and injury distribution but performed with an Area under the Receiver Operating Characteristic (AUROC) curve of 0.700 on a German trauma registry validation. Prediction of Acute Coagulopathy of Trauma (PACT) was developed in USA using six weighted variables (shock index, age, mechanism of injury, Glasgow Coma Scale, cardiopulmonary resuscitation, intubation) and predicted an INR of >1.5 with 73.1% sensitivity and 73.8% specificity. The Bayesian network model is an artificial intelligence system that predicted a prothrombin time ratio of >1.2 based on 14 clinical variables with 90% sensitivity and 92% specificity. Conclusions: The search for ATC prediction models yielded four scoring systems. While there is some potential to be implemented effectively in clinical practice, none have been sufficiently externally validated to demonstrate associations with patient outcomes. These tools remain useful for research purposes to identify populations at risk of ATC.
1. Introduction
Injury is a leading cause of death in the young and middle-aged [1], and uncontrolled haemorrhage is responsible for many of these deaths. Acute traumatic coagulopathy (ATC) is a phenomenon of pathological hypocoagulability post-trauma that is present in about 25% of major trauma patients [2]. The condition has been associated with the excessive activation of the protein C pathway and subsequent reduced activity of coagulation factors and hyperfibrinolysis in addition to decreased clot formation [3]. The development of ATC is correlated strongly with the presence of blunt tissue trauma and hypoperfusion [4].
ATC has been associated with high mortality, particularly when accompanied by hypothermia and acidosis; a difficult to treat state known as the “triad of death” [5]. Currently, diagnosis of ATC is by conventional laboratory coagulation tests, which anecdotally take about 45 min to return, or viscoelastic measures of coagulation, which are not available in all centres. During this time, worsening coagulopathy may contribute to ongoing shock, leading to a vicious cycle and therefore, specific treatment should ideally be started towards prevention and early management of ATC [6]. In contrast to formulaic empirical management of all patients, which may be inefficient and associated with adverse effects, a clinical prediction tool that can identify coagulopathic patients on or before arrival at hospital would be valuable to facilitate such early management.
The aim of this systematic review was to identify published ATC prediction models, evaluate their accuracy and discuss limitations and strengths of each model. We assessed the feasibility of implementing each tool and limitations in study design and model development.
2. Materials and Methods
This systematic review was performed in accordance with the 2015 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [7] (see Supplementary File 1). The study protocol was registered with the International Prospective Register of Systematic Reviews (Prospero) database (registration number: 42018090731). As only published material was used to construct this review, no ethics committee approval was required. Tables describing the included scoring systems and tools are reproduced from their original publications and cited as such.
2.1. Search Strategy
We performed our literature search on February 23rd, 2018. We searched OVID Medline (1946 to Present with Daily Update) and Embase (Embase Classic + Embase 1947 to search date) using a Boolean search strategy. We used Medical Subject Headings (MeSH) terms and keyword searches relating to two broad topics: The population, trauma patients, and the outcome, coagulopathy. We applied a filter to the search to restrict results to predictive, prognostic and observational studies. We combined synonyms with “OR” and concepts with “AND”, and limited the search to studies published in English, as it was beyond the scope of the researchers to translate other languages. The full search strategies for Medline and Embase are available in Appendix A and Appendix B. Grey literature was identified by checking references of eligible studies: Two authors read the reference lists of included articles and screened any potentially relevant articles which had not yet been found for inclusion. Two relevant records were available only as abstracts from conference publications. We contacted the lead authors directly and were supplied with a poster [8] and PhD thesis [9], respectively, for these studies.
2.2. Study Selection
Identified records were scrutinised by two independent reviewers (ST and HG) and evaluated based on pre-discussed inclusion and exclusion criteria during abstract or full article screening. Any discrepancies between the two reviewers were decided by a senior reviewer (MM). We chose to define ATC based on laboratory diagnosis rather than requirement of massive transfusion, as the population of patients with ATC and those requiring massive transfusion are not identical [10]. Risk of bias and concerns about applicability were assessed using the Prediction model study Risk Of Bias ASsessment Tool (PROBAST) [11].
2.3. Inclusion & Exclusion Criteria
Articles were included if they explained the development and/or validation of a scoring system comprised of more than one clinical variable that estimated the likelihood of any trauma patient developing ATC. Single variable studies were not included as they did not reflect scoring systems. Studies pertaining to primarily surgical, cardiac or septic patients were excluded. The outcome of interest was laboratory-based diagnosis of ATC, i.e., coagulopathy defined by International Normalised Ratio (INR), prothrombin time ratio (PTr), activated partial thromboplastin time (aPTT), thromboelastography (TEG) or rotational thromboelastometry (ROTEM) or fibrinogen levels. We included studies with patients 16 years and older.
3. Results
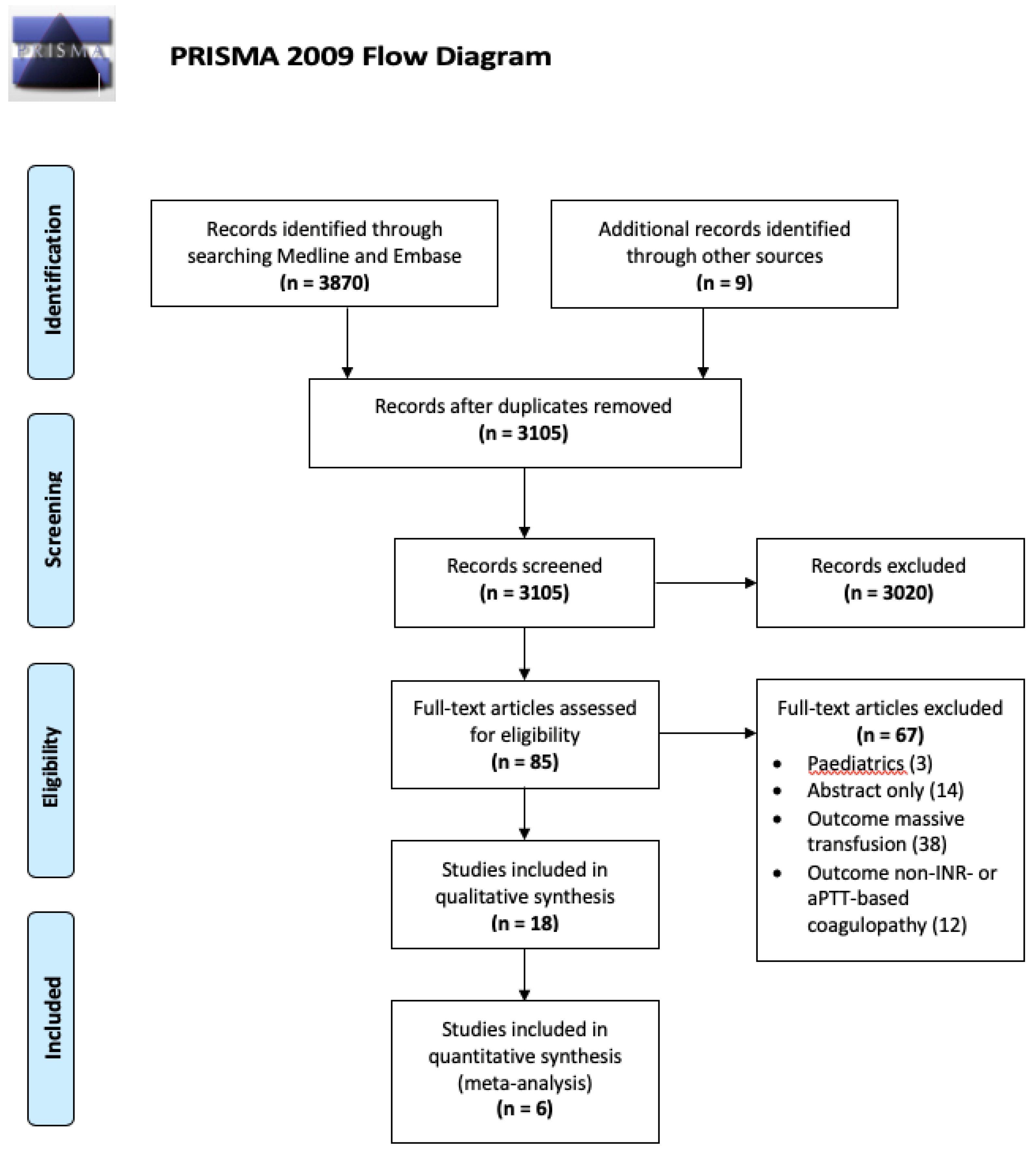
The initial search strategy identified 3096 records after the removal of duplicates. We identified an additional 9 records during text-mining. Through title and abstract screening, we excluded 3020 records. We included 85 articles in full to assess suitability, of which 67 articles were excluded in full text screening for including paediatrics, being only available in abstract or referring to a different outcome. Eighteen articles discussed predictive and associated factors of ATC using the outcome of laboratory-based coagulopathy. Among these, three full text articles described ATC prediction tools, as well as two conference abstracts. One abstract [8] was accompanied by a poster publication which describes an early version of a score also available in full text [12], and the other introduced a score that is discussed in a PhD thesis [9,13]. One additional article described the validation of a scoring system previously produced to predict ATC. Inclusion of the six studies for this review is illustrated in the PRISMA Flow Diagram (Figure 1). Table 1 demonstrates the results of applying the PROBAST to the included studies [14]. A meta-analysis was deemed inappropriate due to the substantial variation in cohorts, outcome definitions and study aims between reported studies.
3.1. Records Identified
3.2. The COAgulopathy of Severe Trauma (COAST) Score
The COAST score, the first prehospital ATC clinical prediction tool to be published, was retrospectively developed on 1680 Australian patients in 2006–08 and prospectively validated in the same centre on 1225 patients in 2009 (Table 3) [16]. Major trauma patients with Injury Severity Score (ISS) >15 requiring urgent surgery, ICU admission, or who died were included and secondary admission, prehospital blood products, or operative management and incomplete data were exclusion criteria. ATC was defined as INR > 1.5 or aPTT > 60 s and the prevalence of ATC was 9.0% and 8.2% in the development and validation cohorts, respectively.
3.3. SBP: Systolic Blood Pressure
A score ≥3 points was defined as a positive COAST score, as this represented the best balance between sensitivity and specificity. The COAST score performed on internal validation with 60% sensitivity, 96.4% specificity, 93.3% accuracy and an AUROC of 0.83 (95% CI 0.78–0.88).
3.3.1. Limitations
The tool was developed and validated in the same single centre in Victoria. No external validation has been undertaken. The selection of the predictor variables was not explained. Head injury due to motor vehicle crashes was very common in this population, which may have contributed to head injury being non-predictive of coagulopathy. There were variables associated with coagulopathy that were not included in the score: Prehospital cardiopulmonary resuscitation had an odds ratio of 13.2, (p < 0.001); however, only 20 patients received CPR. Prehospital intubation also conferred increased risk (OR 7.3, p < 0.001), with 154 intubated patients. Chest injury was predictive (OR 1.95, p = 0.001) but was not included because it is difficult to identify and grade the severity of chest injuries in the prehospital setting.
In the derivation cohort, average temperature was 33.4 ± 9.8 °C whereas in the validation cohort it was 36.3 ± 1.2 °C. The large discrepancy and unusually wide standard deviation suggest that missing data may have been incorrectly recorded as 0 or −1 °C. This wide range was not replicated in the prospectively collected validation cohort. In the validation cohort, missing data was dealt with by “listwise deletion of cases”, which was not done in the derivation cohort.
Abdominal or pelvic content injury had to be diagnosed by paramedics without diagnostic machinery. Although the prehospital paramedics were quite accurate [16], a subjective measure is not without problems. A threshold for injury severity, e.g., using the Abbreviated Injury Scale, was not recorded in the score description.
3.3.2. Strengths
The score is simple and can be easily memorised and calculated without technological tools or diagnostic equipment in the prehospital phase, during triage, or soon after arrival in the emergency department (ED). The COAST score had a high specificity at cut-off ≥3 (96.4%), which results in little over-diagnosis. In the validation cohort, correctly identified patients with coagulopathy had significantly worse outcomes, including more urgent surgery (55.0% vs. 25.0%) and higher mortality (53.3% vs. 27.5%) than missed patients, which demonstrated the predictive ability of the COAST score for severe cases.
3.4. Trauma-Induced Coagulopathy Clinical Score (TICCS)
TICCS was developed on a prospective single-centre Belgian cohort of 82 patients in 2012–13 and validated retrospectively on 33,385 cases from the German Trauma Registry (TR-DGU) [17,18]. Included cases were aged ≥16 years with an ISS of >8 and admission to a resuscitation room, excluding secondary admissions or cases without required data. The development patient outcome was either “severe” (TEG/ROTEM-diagnosed coagulopathy OR INR >1.3 OR fibrinogen <1.5 g/L AND all three of persistent hypotension with active bleeding, massive transfusion and surgical or endovascular haemostasis procedure) or “non-severe” (not fulfilling all severe criteria). The score was developed based on the evidence that tissue injury and hypoperfusion are the primary drivers of ATC [3,19]. The score was modified for validation on the TR-DGU and the outcome of interest on this validation was blood transfusion. The original and modified scores are shown in Table 4.
In the development cohort, eight (9.8%) patients were severe. With a cut-off of ≥10, TICCS correctly identified all eight severe cases, but had three false positives. AUROC was 0.98, sensitivity was 100%, specificity 95.9%, positive predictive value (PPV) 71.7% and negative predictive value (NPV) 100%. All of the false positives had laboratory-defined coagulopathy but did not fulfil other “severe” criteria.
In the validation cohort, 12.7% of patients required blood transfusions. With a cut-off of ≥12, TICCS had an AUROC of 0.700 with a PPV of 48.4%, NPV 89.1%, sensitivity 17.7% and specificity 97.3%.
3.4.1. Limitations
The development and validation studies for TICCS had many inconsistencies, including population characteristics, prediction tool variables and measured outcome. In the development study, the inclusion and exclusion criteria were not fully explained. Furthermore, the sample was small and from a single hospital. The population only included blunt trauma patients. The outcome of interest was chosen for its relationship to massive transfusion, not ATC.
The validation study, which was retrospective and therefore more difficult to fit the prediction tool to, was large enough to demonstrate efficacy, but the score demonstrated a lower PPV. In the validation study, only patients with an ISS of >8 were included, unlike in the original study, which had an ISS range of 4–66. Significant modifications were required for the validation, which calls into question the utility of the validation.
3.4.2. Strengths
TICCS is a simple score, can be calculated by paramedics before arrival at the hospital and gives an idea of overall injury severity on arrival. The development of the scoring variables was sound; using knowledge that tissue injury and hypoperfusion are the main drivers of ATC reduces confounding and the impact of chance, particularly in a small development cohort. The validation cohort was large enough that any outcomes were statistically significant, and the retrospective study design minimises selection or detection bias. The high NPV demonstrates the utility of TICCS for ruling out patients’ need for blood transfusions; however, its low PPV indicates the need for combination with another score or test before initiating treatment.
3.5. Prediction of Acute Coagulopathy of Trauma (PACT)
The PACT score was developed on a single-centre prospective cohort of 315 patients but underwent significant changes before a second multi-centre retrospective development study on 1963 patients and subsequent single-centre prospective validation on 285 patients [12]. There were differences in inclusion and exclusion criteria between development and validation cohorts, including packed red blood cells (PRBC) requirement (inclusion), blunt trauma (inclusion), isolated hip fracture (exclusion), prehospital blood transfusion (exclusion) and expected survival <24 h (exclusion). The outcome of interest was an INR of >1.5. The PACT score is shown in Table 5 [12].
At a threshold of ≥196 points for ATC, the PACT score had a sensitivity of 73.1% and specificity of 73.8%. The overall AUROC of the score was 0.74 on the derivation cohort and 0.80 on validation.
3.5.1. Limitations
There were several differences between the derivation and validation populations: The average ISS was 17.3 (standard deviation (SD) 12.0) in derivation and 32.3 (SD 15.1) in validation, a greater proportion of the validation cohort were intubated (50.9% vs. 16.2%) and more patients were coagulopathic (validation = 9.1%, development = 5.9%). This may be as a result of different inclusion criteria or changing guidelines.
In the validation cohort, only patients who had received a blood transfusion were included. In the development cohort, penetrating injuries were not excluded, although the USA has approximately twice as many penetrating injuries as European countries do (7.9% vs. 4.2%) [20,21], and indeed 12% of the development cohort had penetrating trauma.
3.5.2. Strengths
The PACT score is simple and can be calculated pre-hospital, albeit probably not possible for it to be memorised and calculated without an aid. The sample size was maintained in the validation cohort by imputing missing data or using surrogate markers. The score was validated on an independent population and the technicians investigating the INR were blinded to other patient data.
Exclusion criteria in the validation study were thorough; notably, anticoagulated patients and patients with isolated traumatic brain injury (TBI) were excluded, which targeted the outcome to conventional ATC only, not TBI-induced.
3.6. Bayesian Network Model
Perkins et al. developed the Bayesian network model, a predictive system that “learns” the value of variables through artificial intelligence technology, on 600 cases from the Activation of Coagulation and Inflammation in Trauma (ACIT) study, a multi-national prospective cohort study [9]. It was then prospectively validated on 491 cases from three hospitals. Included patients were >15 years old, required trauma team activation and were primary admissions. Cases were excluded if injury was >2 h before arrival, they received >2000mL of prehospital IV fluid, had burns covering >5% total body surface area, were on anticoagulants, declined consent or had liver disease or a bleeding diathesis. ATC was defined as a PTr of >1.2 plus algorithm-recognition and expert opinion. The Bayesian Network Model is described in Table 6.
With sensitivity set at 90%, the model had 82% and 92% specificity on development and validation cohorts, respectively, and an AUROC of 0.927 and 0.964 respectively. Furthermore, a significant difference was evident in outcomes between coagulopathic and non-coagulopathic patients, as shown in Table 7.
The model was also assessed for performance when variables were missing, as is often the case in emergency patients, and the accuracy was not significantly affected. Variables representing hypoperfusion (blood pressure, heart rate, lactate, base deficit and pH) were the most accurate predictors, although the multivariate score was more accurate than any variable alone.
3.6.1. Limitations
This is a strong, well-designed study with few major limitations. Advanced technology was used to develop the tool and the system relies on this technology to function. The Bayesian Network score is calculated using an online calculator. It would not always be possible to calculate this score in the pre-hospital phase because of its reliance on blood gas analysis, however it was included in this review because blood gases are sometimes available before arrival at hospital, and if not, they are likely to be performed immediately upon arrival.
The system “learnt” from the characteristics of the input population, the ACIT study [22]. The population characteristics, while not necessarily universal, are unlikely to be differ substantially from major trauma populations elsewhere in the developed world.
Some of the data points may be unreliable: Temperature was missing in about 40% of cases; and patients who received >2000 mL of IV fluid pre-hospital were excluded, so information pertaining to this population was imputed.
In order to attain a sensitivity of >90%, a lower specificity was accepted for this tool. 80% of the false-positives in the two cohorts were patients with catastrophic head injuries (abbreviated injury scale (AIS) ≥ 5), who had universally bad outcomes regardless of coagulation status.
3.6.2. Strengths
The Bayesian Network model is highly accurate. It is not significantly affected by missing data and has little risk of over-fitting because the predictors were based on prior knowledge rather than database analysis. This is a particular strength because some of the variables may not be available on hospital arrival.
The outcome of interest in this study was specific and thorough—conventional laboratory diagnosis of coagulopathy identified 94.2% of coagulopathic patients, but the remaining 5.8% had normal PTr with other evidence of coagulopathy identified by physicians.
4. Discussion
The studies on prediction tools for ATC were appropriately developed and reported; each article fulfilled most of the criteria on the TRIPOD Statement [15] for good reporting of prognostic models. Adequate statistical analysis and performance testing was undertaken, and limitations to the models were freely discussed by the authors in their publications. Predictors were developed through a combination of clinical and statistical reasoning, although their selection was not always adequately explained.
None of the prediction tools are ready for widespread clinical use, as no model has performed well enough on external validation to justify including it in clinical guidelines. We attempted to assess for publication bias by searching clinicaltrials.gov for unpublished studies but we found no other trials on ATC prediction scores. Prediction models often perform worse on external validation than during development or internal validation [23], so the tools may need slight adjustments for different populations. Excessive altering can invalidate the system: For example, TICCS performed poorly when validated on the TR-DGU possibly because the variables required too much alteration. It was arguably a different score that was being validated. The COAST, TICCS and PACT scores were all suitable to be applied to patients before arrival at the hospital, as they do not require the results of blood tests to be calculated. The Bayesian model, while highly sensitive and specific, requires information that is not available to pre-hospital personnel. This calls into question its utility as an “early” identification tool; although it still provides useful information very early during hospitalisation, it cannot guide pre-hospital administration of tranexamic acid, a treatment for ATC currently under investigation. We included the Bayesian model in our review because of its potential utility in expediting administration of treatment upon arrival in the hospital.
Scores that are developed on small or single-centre cohorts may not generalise well to other populations. TICCS was developed on a small single centre and performed poorly on the large validation cohort. PACT had very different development and validation cohort characteristics but had a multi-centric development. COAST was developed and validated on the same single centre so it requires external validation before being deemed generalizable.
Among the included studies, the decision of whether or not to exclude cases with known, pre-existing coagulation disorders, such as chronic liver disease or anticoagulant therapy, was inconsistent. The PACT score and the Bayesian model excluded these groups, which may produce a purer sample of patients with only “true” ATC, as opposed to injured people with coagulopathy of other aetiology. However, as this information may not be readily available in the pre-hospital or early in-hospital environment, the scores which are adapted to suit any patient presenting after injury, regardless of these factors, may be more useful. Additionally, developing these scores retrospectively eliminates attrition bias and is cheaper and easier to execute than prospective studies.
The issue of how to deal with missing data is significant in all studies as it introduces considerable selection bias to exclude all patients with a missing variable. This is particularly relevant for scores developed retrospectively using registry data [24]. The Bayesian network showed that its accuracy was not affected by missing data points but COAST, TICCS and PACT relied heavily on few variables. Multiple imputation was used in COAST, TICCS and PACT to substitute missing data with imputed data, and this has been previously demonstrated to reduce selection bias [25].
The definition of ATC varied among these studies, and indeed no universal definition exists. However, it has been previously demonstrated that, regardless of the thresholds used, designating a defined threshold for ATC would be beneficial when designing studies on ATC and also when comparing studies in a systematic review. Attempts have been made to do this, but thus far the differing goals and perceptions of ATC (i.e., whether any coagulopathy is significant, or only coagulopathy in combination with severe haemorrhage-related outcomes) have prevented a resolution. An INR of >1.5 or an aPTT of >60 s is a comparatively high threshold for diagnosis of ATC. ATC is often defined by a PTr/INR of >1.2 [13,26,27] or an INR of >1.3, [17,28,29,30,31] and less commonly by an INR of >1.5. [12,16] An APTT-based definition of ATC also varies widely, from >35 s [26] to >60 s [16,32,33]. In a study aiming to identify the most useful threshold [34], 1031 trauma patients who required PRBC transfusion had their INR tested—50% of patients had an INR of >1.2, for whom in-hospital mortality was 18.5% and massive transfusion rate 32.2%; whereas 21% of patients had an INR of >1.5 and they had an in-hospital mortality of 26.5% and massive transfusion rate of 45.2%. This shows that the population with an INR of >1.5 have significantly worse outcomes, however the clinical significance of coagulopathy at an INR of 1.2–1.5 remains unknown. This study is also confounded by only including patients who required PRBCs. The outcome heterogeneity between the studies suggests that a diagnosis of ATC based solely on an INR/aPTT is incomplete and that the outcome should include clinical manifestations of haemorrhagic progression [35]. Many prediction scores exist to predict the requirement of massive transfusion as a pragmatic, management-focussed outcome. The aim of our systematic review was to predict the coagulopathy itself so we chose to use primarily the INR/aPTT as outcomes. Future prediction scores and systematic reviews should consider using a multifactorial outcome which better identifies significant coagulopathy, such as in the Bayesian Network system [9].
Thromboelastography is becoming more common and useful in the diagnosis of ATC but was not used as an outcome because it is not yet ubiquitous in trauma centres. Point-of-care INR tests are also becoming more common but do not correlate sufficiently well with conventional INR tests to be relied upon [36]. Thromboelastography and point-of-care tests may in the future obviate the need for ATC clinical prediction tools, but prediction tools can be cheap, quick and useful. Additionally, measuring blood transfusion rates as the outcome is not specific to ATC, as it does not discriminate between patients who are bleeding but not coagulopathic and those who are coagulopathic. Using a prediction tool calibrated to this outcome would result in over-diagnosis. The Bayesian model combines laboratory tests and clinical findings to avoid missing cases [37]. A combination outcome of clinical and biochemical evidence of coagulopathy is preferable, although more complicated.
The balance between sensitivity and specificity is an issue in developing prediction tools. In COAST, the aim was to identify a group with worse outcomes who may benefit from directed treatment for ATC, therefore high specificity was prioritised. Conversely, the Bayesian model aimed to avoid missing cases so prioritised high sensitivity. This “over-triage” [9] may be harmful as the treatment of ATC using blood products can be expensive or have deleterious effects on people with normal coagulation [10]. However, lower sensitivity can result in under-treatment.
A factor that was very much considered in the development of these tools was the simplicity of its use; if a score is too difficult or time-consuming to calculate in the emergency department, it is not feasible. The COAST score and TICCS are simple enough to be calculated by hand using a short checklist before or upon hospital arrival. PACT is somewhat more complicated but can also be calculated manually. The Bayesian network uses initial ED blood tests and requires the input of variables into an online calculator, making it more complex than other scores.
This systematic review is limited by wide variation between the tools discussed. The cases had different injury severities, inclusion and exclusion criteria, outcomes and goals. Injuries to certain body regions particularly increase risk of coagulopathy; therefore, if more studies were available it would be of interest to stratify by body region. For example, TBI is thought to cause a different form of coagulopathy [38]. TICCS was designed to identify the “severe” patient, as described above, while the other scores looked for just coagulopathy in the post-trauma period. Ideally, we would be able to compare more similar tools; however, with so few ATC prediction tools in publication, we think this review is nevertheless useful.
The high mortality and persistent difficulties in treating ATC make a reliable clinical prediction tool essential. TEG/ROTEM technology is advancing quickly and may soon be the gold standard for diagnosing ATC. Our current reliance on slow laboratory tests is suboptimal. The four clinical prediction tools discussed here, as well as many prediction models for massive transfusion, have been developed around the world, with relatively few attempts to validate the scores on different populations. External validation is vital to minimise selection bias, ensure validity and to improve international consistency in the quality of treatment trauma patients receive. However, prediction scores are unlikely to perform equally well on all populations, particularly when the mechanism of injuries and management protocols vary between countries. Moving forward with the widespread introduction of clinical prediction scores, the most effective route may be for different centres to validate different scores and find one which suits their population. Continuing to develop new scores, which are likely to include similar variables, is an inefficient use of resources. Common themes among scores are markers of hypoperfusion (hypotension, base deficit) and evidence of severe tissue trauma (high ISS, internal bleeding). Using Bayesian technology to develop models may produce the most accurate scores, but they are not the easiest to use and may not yet be appropriate for use.
The purpose of this review was to identify and bring to light existing ATC prediction models, to encourage the validation, implementation and use of effective models and the abandonment of inadequate scores.
5. Conclusions
The ATC prediction models discussed are based on solid evidence and have sound study designs. They have differing levels of accuracy; however, none have been sufficiently validated to be deemed reliable and widely applicable. Validating these tools across multiple large trauma centres, using a common definition of ATC, is the next step in facilitating earlier effective treatment of coagulopathy and reducing trauma mortality.
Supplementary Materials
The following are available online at https://www.mdpi.com/1648-9144/55/10/653/s1, PRISMA 2009 Checklist. The checklist is a guideline for thorough and transparent reporting of selection, synthesis and analysis of studies during systematic reviews and meta-analysis.
Author Contributions
Sophie Thorn and Helge Güting performed the literature search and screened records to identify relevant publications to be included. Sophie Thorn wrote the manuscript with guidance from Marc Maegele and Biswadev Mitra. Russel Gruen provided feedback prior to submission. This manuscript has been approved for submission by all contributing authors.
Funding
This research received no external funding.
Acknowledgments
We would like to thank our colleagues at the Institut für Forschung in der Operativen Medizin, Universität Witten/Herdecke for their help, and Professor Zane Perkins for providing his PhD thesis for analysis in this review.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. OVID Medline search strategy
| 1 | “Trauma*”.ti,ab. |
| 2 | “Injur*”.ti,ab. |
| 3 | Multiple Trauma/ |
| 4 | 1 OR 2 OR 3 |
| 5 | “Predict*”.ti,ab. |
| 6 | Predictive Value of Tests/ |
| 7 | “Scor*”.ti,ab. |
| 8 | “Observ*”.ti,ab. |
| 9 | Observer Variation/ |
| 10 | 5 OR 6 OR 7 OR 8 OR 9 |
| 11 | Blood Coagulation Disorders/ |
| 12 | “Coagulopathy*”.ti,ab. |
| 13 | ((Clot* or Coagulat*) ADJ2 Disorder).ti,ab. |
| 14 | (“INR” or “International Normali?ed Ratio”).ti,ab. |
| 15 | (“PTT” or “aPTT” or “Partial Thromboplastin Time”).ti,ab. |
| 16 | (“Quick Value” or “Quick’s Value”).ti,ab. |
| 17 | (“PT” or “PTr” or “PR” or “Prothrombin Time” or “Prothrombin Ratio”.ti,ab. |
| 18 | (“ROTEM” or “TEG” or “Rotational Thromboelastometry” or “Thromboelastography”).ti,ab. |
| 19 | 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 |
| 20 | 4 AND 10 AND 19 |
| 21 | Limit 20 to Humans |
| 22 | Limit 21 to English language |
| 23 | Limit 22 to yr=”1998-Current” |
Appendix B. OVID Embase search strategy
| 1 | “Trauma*”.ti,ab. |
| 2 | “Injur*”.ti,ab. |
| 3 | multiple trauma/ |
| 4 | 1 OR 2 OR 3 |
| 5 | prediction/ |
| 6 | linkage analysis/ |
| 7 | scoring system/ |
| 8 | predictive value/ |
| 9 | “Predict*”.ti,ab. |
| 10 | “Scor*”.ti,ab. |
| 11 | 5 OR 6 OR 7 OR 8 OR 9 OR 10 |
| 12 | blood clotting disorder/ |
| 13 | “Coagulopathy*”.ti,ab. |
| 14 | ((Clot* or Coagulat*) ADJ2 Disorder).ti,ab. |
| 15 | (“INR” or “International Normali?ed Ratio”).ti,ab. |
| 16 | (“PTT” or “aPTT” or “Partial Thromboplastin Time”).ti,ab. |
| 17 | (“Quick value” or “Quick’s value”).ti,ab. |
| 18 | (“PT” or “PTr” or “PR” or “Prothrombin Time” or “Prothrombin Ratio”).ti,ab. |
| 19 | (“ROTEM” or “TEG” or “Rotational Thromboelastometry” or “Thromboelastography”).ti,ab. |
| 20 | 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 |
| 21 | 4 AND 11 AND 20 |
| 22 | Limit 21 to human |
| 23 | Limit 22 to English language |
| 24 | Limit 23 to yr=”1998-Current” |
References
- Farrow, N.; Gruen, R.; Baker, A.; Friend, M.; Clark, P.; Cameron, P.; Christey, G.; Curtis, K.; Fitzgerald, M.; Judson, R.; et al. Response to the Australian Commission for Safety and Quality in Health Care on the ‘Australian Safety and Quality Goals for Health Care-Consultation Paper’; Australian Trauma Quality Improvement Program, Ed.; National Trauma Research Institute: Melbourne, Australia, 2012. [Google Scholar]
- Davenport, R.; Manson, J.; De’Ath, H.; Platton, S.; Coates, A.; Allard, S.; Hart, D.; Pearse, R.; Pasi, K.J.; MacCallum, P.; et al. Functional definition and characterization of acute traumatic coagulopathy. Crit. Care Med. 2011, 39, 2652–2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, W.Z. Coagulation complications following trauma. Mil. Med. Res. 2016, 3, 35. [Google Scholar] [CrossRef] [PubMed]
- Frith, D.; Goslings, J.C.; Gaarder, C.; Maegele, M.; Cohen, M.J.; Allard, S.; Johansson, P.I.; Stanworth, S.; Thiemermann, C.; Brohi, K. Definition and drivers of acute traumatic coagulopathy: clinical and experimental investigations. J. Thromb. Haemost. 2010, 8, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; Tullio, F.; Cameron, P.A.; Fitzgerald, M. Trauma patients with the ‘triad of death’. Emerg. Med. J. 2012, 29, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Eddy, V.A.; Morris, J.A.; Cullinane, D.C. Hypothermia, coagulopathy, and acidosis. Surg. Clin. N. Am. 2000, 80, 845–854. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- Peltan, I.D.; Vande Vusse, L.K.; Caldwell, E.; Rowhani-Rahbar, A.; Maier, R.V.; Watkins, T.R. A prehospital prediction tool for acute traumatic coagulopathy. In Proceedings of the American Thoracic Society International Conference, ATS, Denver, CO, USA, 15–20 May 2015; Volume 191. [Google Scholar]
- Perkins, Z. Bayesian Network Decision-Support for Severe Lower Limb Trauma. Ph.D. Thesis, Queen Mary, University of London, London, UK, 2016. [Google Scholar]
- Mitra, B.; Cameron, P.A.; Gruen, R.L. Aggressive fresh frozen plasma (FFP) with massive blood transfusion in the absence of acute traumatic coagulopathy. Injury 2012, 43, 33–37. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 June 2018).
- Peltan, I.D.; Rowhani-Rahbar, A.; Vusse, L.K.V.; Caldwell, E.; Rea, T.D.; Maier, R.V.; Watkins, T.R. Development and validation of a prehospital prediction model for acute traumatic coagulopathy. Crit. Care 2016, 20, 371. [Google Scholar] [CrossRef]
- Perkins, Z.; Yet, B.; Glasgow, S.; Brohi, K.; Marsh, W.; Tai, N.R.M. Early prediction of traumatic coagulopathy using admission clinical variables. Shock 2013, 40, 25. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; The Prediction model Risk Of Bias ASsessment Tool (PROBAST) Group. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, B.; Cameron, P.A.; Mori, A.; Maini, A.; Fitzgerald, M.; Paul, E.; Street, A. Early prediction of acute traumatic coagulopathy. Resuscitation 2011, 82, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Tonglet, M.L.; Minon, J.M.; Seidel, L.; Poplavsky, J.L.; Vergnion, M. Prehospital identification of trauma patients with early acute coagulopathy and massive bleeding: results of a prospective non-interventional clinical trial evaluating the Trauma Induced Coagulopathy Clinical Score (TICCS). Crit. Care 2014, 18, 648. [Google Scholar] [CrossRef] [PubMed]
- Tonglet, M.; Lefering, R.; Minon, J.M.; Ghuysen, A.; D’Orio, V.; Hildebrand, F.; Pape, H.C.; Horst, K. Prehospital identification of trauma patients requiring transfusion: results of a retrospective study evaluating the use of the trauma induced coagulopathy clinical score (TICCS) in 33,385 patients from the TraumaRegister DGU. Acta Chir. Belg. 2017, 117, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Davenport, R. Pathogenesis of acute traumatic coagulopathy. Transfusion 2013, 53 (Suppl. 1), 23s–27s. [Google Scholar] [CrossRef] [PubMed]
- Glance, L.G.; Osler, T.M.; Dick, A.W.; Mukamel, D.B.; Meredith, W. The Survival Measurement and Reporting Trial for Trauma (SMARTT): Background and Study Design. J. Trauma: Inj. Infect. Crit. Care 2010, 68, 1491–1497. [Google Scholar] [CrossRef]
- Edwards, A.; Di Bartolomeo, S.; Chieregato, A.; Coats, T.; Della Corte, F.; Giannoudis, P.; Gomes, E.; Groenborg, H.; Lefering, R.; Leppaniemi, A.; et al. A comparison of European Trauma Registries. The first report from the EuroTARN Group. Resuscitation 2007, 75, 286–297. [Google Scholar]
- Constantinou, A.C.; Fenton, N.; Marsh, W.; Radlinski, L. From complex questionnaire and interviewing data to intelligent Bayesian network models for medical decision support. Artif. Intell. Med. 2016, 67, 75–93. [Google Scholar] [CrossRef]
- Han, K.; Song, K.; Choi, B.W. How to Develop, Validate, and Compare Clinical Prediction Models Involving Radiological Parameters: Study Design and Statistical Methods. Korean J. Radiol. 2016, 17, 339–350. [Google Scholar] [CrossRef]
- Shivasabesan, G.; Mitra, B.; O’Reilly, G.M. Missing data in trauma registries: A systematic review. Injury 2018, 49, 1641–1647. [Google Scholar] [CrossRef]
- O’Reilly, G.M.; Cameron, P.A.; Jolley, D.J. Which patients have missing data? An analysis of missingness in a trauma registry. Injury 2012, 43, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Genét, G.F.; Johansson, P.I.; Meyer, M.A.S.; Sølbeck, S.; Sørensen, A.M.; Larsen, C.F.; Welling, K.L.; Windeløv, N.A.; Rasmussen, L.S.; Ostrowski, S.R. Trauma-Induced Coagulopathy: Standard Coagulation Tests, Biomarkers of Coagulopathy, and Endothelial Damage in Patients with Traumatic Brain Injury. J. Neurotrauma 2013, 30, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Cheddie, S.; Muckart, D.J.J.; Hardcastle, T.C. Base deficit as an early marker of coagulopathy in trauma. S. Afr. J. Surg. 2013, 51, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, M.E.; Howard, B.M.; Sperry, J.L.; Hubbard, A.E.; Decker, A.L.; Cuschieri, J.; Minei, J.P.; Moore, E.E.; Brownstein, B.H.; Maier, R.V.; et al. Evolving beyond the vicious triad: Differential mediation of traumatic coagulopathy by injury, shock, and resuscitation. J. Trauma Acute Care Surg. 2015, 78, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.J.; Kutcher, M.; Redick, B.; Nelson, M.; Call, M.; Knudson, M.; Schreiber, M.A.; Bulger, E.M.; Muskat, P.; Alarcon, L.H.; et al. Clinical and mechanistic drivers of acute traumatic coagulopathy. J. Trauma Acute Care Surg. 2013, 75, S40–S47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engels, P.T.; Rezende-Neto, J.B.; Al Mahroos, M.; Scarpelini, S.; Rizoli, S.B.; Tien, H.C. The natural history of trauma-related coagulopathy: implications for treatment. J. Trauma Inj. Infect. Crit. Care 2011, 71, S448–S455. [Google Scholar] [CrossRef] [PubMed]
- Wafaisade, A.; Wutzler, S.; Lefering, R.; Tjardes, T.; Banerjee, M.; Paffrath, T.; Bouillon, B.; Maegele, M. Trauma Registry of the Deutsche Gesellschaft für Unfallchirurgie. Drivers of acute coagulopathy after severe trauma: a multivariate analysis of 1987 patients. Emerg. Med. J. 2010, 27, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.-X.; Wang, L.; Zhou, G.-J.; Zhang, M.; Gan, J.-X. Risk factors and clinical significance of trauma-induced coagulopathy in ICU patients with severe trauma. Eur. J. Emerg. Med. 2013, 20, 286–290. [Google Scholar] [CrossRef]
- Brohi, K.; Singh, J.; Heron, M.; Coats, T. Acute traumatic coagulopathy. J. Trauma Acute Care Surg. 2003, 54, 1127–1130. [Google Scholar] [CrossRef]
- Peltan, I.D.; Vusse, L.K.V.; Maier, R.V.; Watkins, T.R. An INR-based definition of acute traumatic coagulopathy is associated with mortality, venous thromboembolism, and multiple organ failure after injury. Crit. Care Med. 2015, 43, 1429–1438. [Google Scholar] [CrossRef]
- Palmer, L.; Martin, L. Traumatic coagulopathy--part 1: Pathophysiology and diagnosis. J. Vet. Emerg. Crit. Care (San Antonio) 2014, 24, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; O’Reilly, G.; Collecutt, M.; A Cameron, P.; Phillips, L.; Davis, A. Prospective comparison of point-of-care international normalised ratio measurement versus plasma international normalised ratio for acute traumatic coagulopathy. Emerg. Med. Australas. 2012, 24, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Grimes, D.A.; Schulz, K.F. Surrogate End Points in Clinical Research: Hazardous to Your Health. Obstet. Gynecol. 2005, 105, 1114–1118. [Google Scholar] [CrossRef]
- Kumar, M.A. Coagulopathy Associated with Traumatic Brain Injury. Curr. Neurol. Neurosci. Rep. 2013, 13, 391. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram demonstrating the inclusion and exclusion process undertaken.


{kind=link}
Table 1.
PROBAST results.
| Study | Risk of Bias | Applicability | Overall | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Participants | Predictors | Outcome | Analysis | Participants | Predictors | Outcome | ROB | Applicability | |
| COAST | + | + | + | + | + | + | + | + | + |
| TICCS 1 | − | + | + | − | + | + | ? | − | ? |
| TICCS 2 | + | + | + | + | + | + | + | + | + |
| PACT 1 | + | + | + | ? | + | + | + | ? | + |
| PACT 2 | + | + | + | + | + | + | + | + | + |
| Perkins | + | + | + | + | + | + | + | + | + |
PROBAST—Prediction model Risk of Bias Assessment Tool; ROB—risk of bias. + indicates low ROB/low concern regarding applicability; − indicates high ROB/high concern regarding applicability; ? indicates unclear ROB/unclear concern regarding applicability.
Table 2.
Relevant records identified on systematic literature search.
| Name (year) | Score | Purpose | Score Variables | Development/Validation Patient No. | Cohort | Outcome | Sensitivity Specificity AUROC |
|---|---|---|---|---|---|---|---|
| Mitra (2011) [16] | COAST (COAgulopathy of Severe Trauma) | Retrospective cohort analysis (development) and prospective cohort study (validation) | Entrapment Prehospital SBP Temperature Chest decompression Abdominal or pelvic injury | 1680/1225 | Single level 1 trauma centre Victoria, Australia | INR >1.5 or aPTT >60 s | 60.0% 96.4% 0.83 |
| Perkins (2013) [9] PhD thesis | Bayesian network model | Retrospective cohort analysis (development) and prospective and retrospective cohort analyses (validation) | HR Temperature SBP Haemothorax FAST Pelvic or long bone fracture GCS Lactate Base deficit pH Injury mechanism and energy IV fluid volume | 600/373 | Activation of Coagulation and Inflammation in Trauma study cohort in London, UK (development) and a trauma centre in Oxford, UK, and Cologne, Germany (validation) | PTr >1.2 | 90.0% 92.0% 0.96 |
| Tonglet (2014) [17] | TICCS (Trauma-Induced Coagulopathy Clinical Score) | Prospective non-controlled observational clinical study | Resuscitation room admission SBP Distribution of injuries | 82/– | Single level 1 trauma centre in Liège, Belgium | INR >1.3 or fibrinogen <1.5 or ROTEM-defined coagulopathy | 100% 95.9% 0.98 |
| Peltan (2015) [8] Poster | PACT (Prediction of Acute Traumatic Coagulopathy) | Prospective cohort study | Shock index Injury-to-ED time White race Age First GCS First RR | 324/– | Single level 1 trauma centre in Washington, USA | INR ≥1.5 | 73% 74% 0.79 |
| Peltan (2016) [12] | PACT | Retrospective cohort analysis (development) and prospective cohort study (validation) | Shock index Age GCS Mechanism of injury Intubation CPR | 1963/285 | 44 trauma centres on the Oregon Trauma Registry | INR >1.5 | 73.1% 73.8% 0.74 |
| Tonglet (2017) [18] | TICCS | Retrospective cohort analysis | Admission to resuscitation room SBP Distribution of injuries | –/33,385 | Over 600 trauma centres on the German Trauma Registry | Blood transfusion | 48.4% 89.1% 0.83 |
Important information on each publication is summarised here. AUROC—Area under the Receiver Operating Characteristic Curve. SBP—systolic blood pressure; INR—International Normalised Ratio; aPTT—activated Partial Thromboplastin Time; HR—heart rate; FAST—Focused Assessment with Sonography in Trauma; GCS—Glasgow Coma Scale; PTr—prothrombin ratio; ROTEM—rotational thromboelastometry; ED—emergency department; RR—respiratory rate; CPR—cardiopulmonary resuscitation.
Table 3.
The COAgulopathy of Severe Trauma (COAST) score.
| Variable | Value | Score |
|---|---|---|
| Entrapment | Yes | 1 |
| Systolic blood pressure (SBP) | <100 mmHg <90 mmHg | 1 2 |
| Temperature | <35 °C <32 °C | 1 2 |
| Chest decompression | Yes | 1 |
| Abdominal or pelvic content injury | Yes | 1 |
| Highest total possible | 7 |
Table 4.
The original and modified Trauma-Induced Coagulopathy Clinical Score (TICCS) score.
| Original Criteria | Points | Modified Criteria | Points |
|---|---|---|---|
| General severity Admitted to resus room Regular ED room | 2 0 | General severity Admitted to resus room | 2 |
| Blood pressure <90 at least once Always >90mmHg | 5 0 | Blood pressure <90 at least once Always >90mmHg | 5 0 |
| Significant injuries Head/neck L upper extremity R upper extremity L lower extremity R lower extremity Torso Abdomen Pelvis | 1 1 1 1 1 2 2 2 | Significant injuries (AIS ≥3) Head/neck Upper extremity Lower extremity Torso Abdomen Pelvis | 1 1 1 2 2 2 |
| Total possible score | 0–18 | Total possible score | 2–16 |
ED—emergency department; resus room—resuscitation room; AIS—Abbreviated Injury Scale; R—right; L—left.
Table 5.
The PACT Score.
| Variable | Value | Points Per Unit |
|---|---|---|
| Prehospital shock index ≥1 | Yes/no | 90 |
| Age | Years to nearest decade | 1 |
| Mechanism of injury not motor vehicle, motorcycle or bicycle crash | Yes/no | 50 |
| Number of GCS points below 15 | 15-GCS | 7 |
| Prehospital CPR | Yes/no | 120 |
| Prehospital intubation | Yes/no | 50 |
| Total possible points | - | 394 + age |
Shock index—heart rate/systolic blood pressure; GCS—Glasgow Coma Scale; CPR—cardiopulmonary resuscitation.
Table 6.
The Bayesian Network Model.
| Variable | Value |
|---|---|
| Heart rate | Beats per minute |
| Systolic blood pressure | mmHg |
| Temperature | ≥34 °C or <34 °C |
| Haemothorax | Present (suspected, or on CXR) or absent |
| FAST | Positive for abdominal free fluid or negative |
| Unstable pelvic fracture | Present (suspected, or on PXR) or absent |
| Long bone (femur, tibia, humerus) fracture | Present (suspected) or absent |
| GCS | On admission or prior to intubation |
| Lactate | On arterial or venous blood gas analysis |
| Base deficit | On arterial or venous blood gas analysis |
| pH | On arterial or venous blood gas analysis |
| Mechanism of injury | Blunt or penetrating |
| Energy | High (gun-shot wound, fall >6 m, vehicular mechanism, entrapment, crush or blast) or low (stab, other blunt injury, low-velocity gun-shot) |
| Volume of fluid administered | <500 mL or 500–2000 mL or >2000 mL crystalloid or colloid |
CXR—chest x-ray; FAST—focused assessment with sonography in trauma; PXR—pelvic x-ray; GCS—Glasgow Coma Scale.
Table 7.
Outcomes in the development and validation cohorts analysed for the Bayesian Network Model.
Table 7.
Outcomes in the development and validation cohorts analysed for the Bayesian Network Model.
| Development | Validation | |||
|---|---|---|---|---|
| Outcome | Coagulopathy | No Coagulopathy | Coagulopathy | No Coagulopathy |
| 24-hour mortality | 36.6% | 1.3% | 24.5% | 0.2% |
| In-hospital mortality | 53.7% | 5.6% | 49.1% | 5.2% |
| Blood transfusion | 90.1% | 23.2% | 96.2% | 16.0% |
| Massive transfusion* | 40.9% | 1.3% | 47.2% | 0.9% |
* Massive transfusion is defined as ≥10 units of packed red blood cells within 24 hours.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Thorn, S.; Güting, H.; Maegele, M.; Gruen, R.L.; Mitra, B. Early Identification of Acute Traumatic Coagulopathy Using Clinical Prediction Tools: A Systematic Review. Medicina 2019, 55, 653. https://doi.org/10.3390/medicina55100653
AMA Style
Thorn S, Güting H, Maegele M, Gruen RL, Mitra B. Early Identification of Acute Traumatic Coagulopathy Using Clinical Prediction Tools: A Systematic Review. Medicina. 2019; 55(10):653. https://doi.org/10.3390/medicina55100653
Chicago/Turabian StyleThorn, Sophie, Helge Güting, Marc Maegele, Russell L. Gruen, and Biswadev Mitra. 2019. "Early Identification of Acute Traumatic Coagulopathy Using Clinical Prediction Tools: A Systematic Review" Medicina 55, no. 10: 653. https://doi.org/10.3390/medicina55100653