
Abstract
Purpose
Evaluation of patient radiation exposure during uterine artery embolization (UAE) and literature review to identify techniques minimizing required dose.
Methods
A total of 224 of all included 286 (78 %) women underwent UAE according to a standard UAE-protocol (bilateral UAE from unilateral approach using a Rösch inferior mesenteric and a microcatheter, no aortography, no ovarian artery catheterization or embolization) and were analyzed for radiation exposure. Treatment was performed on three different generations of angiography systems: (I) new generation flat-panel detector (N = 108/151); (II) classical image amplifier and pulsed fluoroscopy (N = 79/98); (III) classical image amplifier and continuous fluoroscopy (N = 37/37). Fluoroscopy time (FT) and dose-area product (DAP) were documented. Whenever possible, the following dose-saving measures were applied: optimized source-object, source-image, and object-image distances, pulsed fluoroscopy, angiographic runs in posterior-anterior direction with 0.5 frames per second, no magnification, tight collimation, no additional aortography.
Results
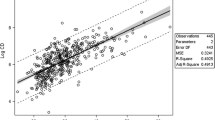
In a standard bilateral UAE, the use of the new generation flat-panel detector in group I led to a significantly lower DAP of 3,156 cGy × cm2 (544–45,980) compared with 4,000 cGy × cm2 (1,400–13,000) in group II (P = 0.033). Both doses were significantly lower than those of group III with 8,547 cGy × cm2 (3,324–35,729; P < 0.001). Other reasons for dose escalation were longer FT due to difficult anatomy or a large leiomyoma load, additional angiographic runs, supplementary ovarian artery embolization, and obesity.
Conclusions
The use of modern angiographic units with flat panel detectors and strict application of methods of radiation reduction lead to a significantly lower radiation exposure. Target DAP for UAE should be kept below 5,000 cGy × cm2.
Similar content being viewed by others


References
Freed MM, Spies JB (2010) Uterine artery embolization for fibroids: a review of current outcomes. Semin Reprod Med 28:235–241
Poulsen B, Munk T, Ravn P (2011) Long-term follow up after uterine artery embolization for symptomatic uterine leiomyomas. Acta Obstet Gynecol Scand 90:1281–1283
Spies JB, Bruno J, Czeyda-Pommersheim F et al (2005) Long-term outcome of uterine artery embolization of leiomyomata. Obstet Gynecol 106:933–939
Lohle PNM, Voogt MJ, De Vries J et al (2008) Long-term outcome of uterine artery embolization for symptomatic uterine leiomyomas. J Vasc Interv Radiol 19:319–326
Scheurig-Muenkler C, Koesters C, Powerski MJ et al (2013) Clinical long-term outcome after uterine artery embolization: sustained symptom control and improvement of quality of life. J Vasc Interv Radiol 24:765–771
Moss JG, Cooper KG, Khaund A et al (2011) Randomised comparison of uterine artery embolisation (UAE) with surgical treatment in patients with symptomatic uterine fibroids (REST trial): 5-year results. BJOG 118:936–944
Broder MS, Goodwin S, Chen G et al (2002) Comparison of long-term outcomes of myomectomy and uterine artery embolization. Obstet Gynecol 100:864–868
Pinto I, Chimeno P, Romo A et al (2003) Uterine fibroids: uterine artery embolization versus abdominal hysterectomy for treatment–a prospective, randomized, and controlled clinical trial. Radiology 226:425–431
Siskin GP, Shlansky-Goldberg RD, Goodwin SC et al (2006) A prospective multicenter comparative study between myomectomy and uterine artery embolization with polyvinyl alcohol microspheres: long-term clinical outcomes in patients with symptomatic uterine fibroids. J Vasc Interv Radiol 17:1287–1295
Hirst A, Dutton S, Wu O et al (2008) A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids: the HOPEFUL study. Health Technol Assess 12(5):1–248
Van der Kooij SM, Hehenkamp WJK, Volkers NA et al (2010) Uterine artery embolization vs hysterectomy in the treatment of symptomatic uterine fibroids: 5-year outcome from the randomized EMMY trial. Am J Obstet Gynecol 203(105):e1–e13
Tropeano G, Di Stasi C, Amoroso S et al (2010) Long-term effects of uterine fibroid embolization on ovarian reserve: a prospective cohort study. Fertil Steril 94:2296–2300
McLucas B, Danzer H, Wambach C et al (2013) Ovarian reserve following uterine artery embolization in women of reproductive age: a preliminary report. Minim Invasive Ther Allied Technol 22:45–49
Katsumori T, Kasahara T, Tsuchida Y et al (2008) Amenorrhea and resumption of menstruation after uterine artery embolization for fibroids. Int J Gynaecol Obstet 103:217–221
Tse G, Spies JB (2010) Radiation exposure and uterine artery embolization: current risks and risk reduction. Tech Vasc Interv Radiol 13:148–153
Andrews RT, Brown PH (2000) Uterine arterial embolization: factors influencing patient radiation exposure. Radiology 217:713–722
Vetter S, Schultz FW, Strecker E-P et al (2004) Patient radiation exposure in uterine artery embolization of leiomyomata: calculation of organ doses and effective dose. Eur Radiol 14:842–848
Glomset O, Hellesnes J, Heimland N et al (2006) Assessment of organ radiation dose associated with uterine artery embolization. Acta Radiol 47:179–185
Nishizawa K, Masuda Y, Morinaga K et al (2008) Surface dose measurement in patients and physicians and effective dose estimation in patients during uterine artery embolisation. Radiat Prot Dosimetry 128:343–350
Sapoval M, Pellerin O, Rehel J-L et al (2010) Uterine artery embolization for leiomyomata: optimization of the radiation dose to the patient using a flat-panel detector angiographic suite. Cardiovasc Intervent Radiol 33:949–954
Nikolic B, Spies JB, Lundsten MJ et al (2000) Patient radiation dose associated with uterine artery embolization. Radiology 214:121–125
Kröncke TJ, Gauruder-Burmester A, Gronewold M et al (2004) Technical success rate, peri-interventional complications and radiation exposure of the transarterial embolization for leiomyomas of the uterus. Rofo 176:580–589
Vetter S, Schultz FW, Strecker E-P et al (2005) Optimisation strategies and justification: an example in uterine artery embolisation for fibroids. Radiat Prot Dosimetry 117:50–53
Bratby MJ, Ramachandran N, Sheppard N et al (2007) Prospective study of elective bilateral versus unilateral femoral arterial puncture for uterine artery embolization. Cardiovasc Intervent Radiol 30:1139–1143
White AM, Banovac F, Spies JB (2007) Patient radiation exposure during uterine fibroid embolization and the dose attributable to aortography. J Vasc Interv Radiol 18:573–576
Naguib NNN, Nour-Eldin N-EA, Lehnert T et al (2009) Uterine artery embolization: optimization with preprocedural prediction of the best tube angle obliquity by using 3D-reconstructed contrast-enhanced MR angiography. Radiology 251:788–795
Costantino M, Lee J, McCullough M et al (2010) Bilateral versus unilateral femoral access for uterine artery embolization: results of a randomized comparative trial. J Vasc Interv Radiol 21:829–835 quiz 835
Maleux G, Michielsen K, Timmerman D et al (2013) 2D versus 3D roadmap for uterine artery catheterization: impact on several angiographic parameters. Acta Radiol 55(1):62–70
Gupta A, Grünhagen T, Live MR (2013) angiographic roadmapping for uterine artery embolization: a feasibility study. J Vasc Interv Radiol 24:1690–1697
White AM, Banovac F, Yousefi S et al (2007) Uterine fibroid embolization: the utility of aortography in detecting ovarian artery collateral supply. Radiology 244:291–298
Binkert CA, Andrews RT, Kaufman JA (2001) Utility of nonselective abdominal aortography in demonstrating ovarian artery collaterals in patients undergoing uterine artery embolization for fibroids. J Vasc Interv Radiol 12:841–845
Kroencke TJ, Scheurig C, Kluner C et al (2006) Uterine fibroids: contrast-enhanced MR angiography to predict ovarian artery supply–initial experience. Radiology 241:181–189
Gupta A, Zuurmond K, Grünhagen T et al (2012) Three-dimensional rotational angiography is preferable to conventional two-dimensional techniques for uterine artery embolization. Diagn Interv Radiol 19:418–422
Conflict of interest
The authors certify that there is no actual or potential conflict of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Scheurig-Muenkler, C., Powerski, M.J., Mueller, JC. et al. Radiation Exposure During Uterine Artery Embolization: Effective Measures to Minimize Dose to the Patient. Cardiovasc Intervent Radiol 38, 613–622 (2015). https://doi.org/10.1007/s00270-014-0962-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-014-0962-6