
Abstract
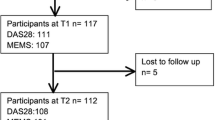
Medication adherence is believed to be a major contributor to treatment outcomes yet studies quantifying this relationship as rare in rheumatoid arthritis (RA). To determine the association of adherence to DMARD therapy with treatment outcomes among new and existing DMARD users over 2 years. Relevant clinical parameters were obtained from a longitudinal cohort of RA patients, most of who were treated with combination therapy. Patients were classified as adherent if the proportion of days covered for each DMARD was ≥80%. Outcome measures were the change in the disease activity score in 28 joints (DAS28), simplified disease activity index (SDAI), modified health assessment questionnaires (mHAQ) and proportion of patients who achieved response criteria. An inverse propensity-score weighting method was used to estimate the association of adherence with each outcome. Of 194 patients invited, a total of 111 patients (new = 45 and existing = 66 DMARD users) met study eligibility. DMARD-naive patients demonstrated relatively higher rates of adherence compared to existing users. After controlling for confounding variables, adherence was significantly associated with reduction in DAS28 (β = −1.5, 95% CI of β = − 2.17 to −0.83, p < 0.0001), SDAI (β = −9.44, 95% CI of β = −15.53 to −3.35, p = 0.002) and mHAQ (β = −0.269, 95% CI of β, −0.462 to −0.077, p = 0.017) over 2 years among new patients and adherent patients were more likely to achieve most response criteria compared to non-adherent patients. Such associations were not replicated among existing DMARD users. Adherence to combination DMARD therapy was associated with improvements in disease activity and functional outcomes in the first 2 years of therapy.
Similar content being viewed by others

References
Wabe N, Wiese MD (2016) Treating rheumatoid arthritis to target: physician and patient adherence issues in contemporary rheumatoid arthritis therapy. J Eval Clin Pract. doi:10.1111/jep.12620 (Epub ahead of print)
Salt E, Frazier SK (2010) Adherence to disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a narrative review of the literature. Orthop Nurs 29:260–275
Blum MA, Koo D, Doshi JA (2011) Measurement and rates of persistence with and adherence to biologics for rheumatoid arthritis: a systematic review. Clin Ther 33:901–913
Tamás K (2010) Clinical and pharmacoeconomic impact of patient medication adherence. Dissertation, Semmelweis University
DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW (2002) Patient adherence and medical treatment outcomes: a meta-analysis. Med Care 40:794–811
Cannon GW, Mikuls TR, Hayden CL et al (2011) Merging Veterans Affairs rheumatoid arthritis registry and pharmacy data to assess methotrexate adherence and disease activity in clinical practice. Arthritis Care Res (Hoboken) 63:1680–1690
Pasma A, Schenk CV, Timman R et al (2015) Non-adherence to disease-modifying antirheumatic drugs is associated with higher disease activity in early arthritis patients in the first year of the disease. Arthritis Res Ther 17:281
Bluett J, Morgan C, Thurston L et al (2015) Impact of inadequate adherence on response to subcutaneously administered anti-tumour necrosis factor drugs: results from the Biologics in rheumatoid arthritis genetics and genomics study syndicate cohort. Rheumatology (Oxford) 54:494–499
Smolen JS, Aletaha D, Bijlsma JW et al (2010) Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis 69:631–637
Wabe N, Sorich M, Wechalekar M et al (2015) Characterising deviation from treat-to-target strategies for early rheumatoid arthritis: the first three years. Arthritis Res Ther 17:48
Wabe N, Sorich MJ, Wechalekar MD et al (2016) Drug-induced toxicity and patient reported outcomes in rheumatoid arthritis patients following intensive treated-to-target strategy: does ceasing therapy due to toxicity worsen outcomes in long term? Int J Clin Pract 70:340–350
Wabe N, Sorich MJ, Wechalekar MD et al (2015) Determining the acceptable level of physician compliance with a treat-to-target strategy in early rheumatoid arthritis. Int J Rheum Dis. doi:10.1111/1756-185X.12816 (Epub ahead of print)
Proudman SM, Keen HI, Stamp LK et al (2007) Response-driven combination therapy with conventional disease-modifying antirheumatic drugs can achieve high response rates in early rheumatoid arthritis with minimal glucocorticoid and nonsteroidal anti-inflammatory drug use. Semin Arthritis Rheum 37:99–111
Pincus T, Summey JA, Soraci SA Jr et al (1983) Assessment of patient satisfaction in activities of daily living using a modified Stanford Health Assessment Questionnaire. Arthritis Rheum 26:1346–1353
DeVellis RF, Callahan LF (1993) A brief measure of helplessness in rheumatic disease: the helplessness subscale of the Rheumatology Attitudes Index. J Rheumatol 20:866–869
Wells G, Becker JC, Teng J et al (2009) Validation of the 28-joint disease activity score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann Rheum Dis 68:954–960
Smolen J, Breedveld F, Schiff M et al (2003) A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 42:244–257
Choudhry NK, Shrank WH, Levin RL et al (2009) Measuring concurrent adherence to multiple related medications. Am J Manag Care 15:457–464
Van Gestel A, Prevoo M, Van’t Hof M et al (1996) Development and validation of the European League Against Rheumatism response criteria for rheumatoid arthritis: comparison with the preliminary American College of Rheumatology and the World Health Organization/International League Against Rheumatism criteria. Arthritis Rheum 39:34–40
Kosinski M, Zhao SZ, Dedhiya S et al (2000) Determining minimally important changes in generic and disease-specific health-related quality of life questionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum 43:1478–1487
Austin PC (2011) An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 46: 399–424
Austin PC, Stuart EA (2015) Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med 34:3661–3679
Wabe NT, Sorich MJ, Wechalekar MD et al (2016) Effect of adherence to protocolized targeted intensifications of disease-modifying antirheumatic drugs on treatment outcomes in rheumatoid arthritis: results from an australian early arthritis cohort. J Rheumatol 43:1643–1649
Barnabe C, Sun Y, Boire G et al (2015) Heterogeneous disease trajectories explain variable radiographic, function and quality of life outcomes in the Canadian early arthritis cohort (CATCH). PloS one 10:e0135327
Siemons L, Ten Klooster PM, Vonkeman HE et al (2014) Distinct trajectories of disease activity over the first year in early rheumatoid arthritis patients following a treat-to-target strategy. Arthritis Care Res (Hoboken) 66:625–630
Quinn MA, Emery P (2003) Window of opportunity in early rheumatoid arthritis: possibility of altering the disease process with early intervention. Clin Exp Rheumatol 21:S154–S157
Jimmy B, Jose J (2011) Patient medication adherence: measures in daily practice. Oman Med J 26:155–159
McCaffrey DF, Griffin BA, Almirall D et al (2013) A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med 32:3388–3414
Yu AP, Yu YF, Nichol MB (2010) Estimating the effect of medication adherence on health outcomes among patients with type 2 diabetes—an application of marginal structural models. Value Health 13:1038–1045
Acknowledgements
The authors are grateful to all rheumatologists and rheumatology nurses involved in the treatment and care of patients as well as patients who participated in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The authors had no financial support or other benefits from commercial sources for the work reported in the manuscript, or any other financial interests that could create a potential conflict of interest or the appearance of a conflict of interest with regard to the work.
Conflict of interest
The authors have no competing interests to report.
Ethical approval
Ethics approval was obtained from the University of South Australia (protocol no.0000031928) and the Royal Adelaide Hospital (protocol no.140303) for the longitudinal observational cohort and for the linkage of prescribing data.
Electronic supplementary material
Below is the link to the electronic supplementary material.
296_2017_3655_MOESM3_ESM.tif
The rate of medication adherence according to different definitions of adherence:*P<0.05 for DMARD-naïve vs experienced patients; PDC, proportion of days covered; PDC-1, adherence of ≥80% with at least one DMARD; PDC-average, average PDC≥80%; PDC-all, PDC≥80% for all DMARDs (TIF 168 KB)
296_2017_3655_MOESM4_ESM.tif
Proportion of patients who achieved EULAR and SDAI response criteria and MCID for mHAQ stratified according to treatment status:*P<0.0001 for DMARD-naïve vs experienced patients; EULAR, European League Against Rheumatism; SDAI, Simplified disease activity index; MCID, minimally clinically important differences, mHAQ, modified health assessment questionaries (TIF 204 KB)
Rights and permissions
About this article

Cite this article
Wabe, N., Lee, A., Wechalekar, M. et al. Adherence to combination DMARD therapy and treatment outcomes in rheumatoid arthritis: a longitudinal study of new and existing DMARD users. Rheumatol Int 37, 897–904 (2017). https://doi.org/10.1007/s00296-017-3655-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3655-z