
Summary
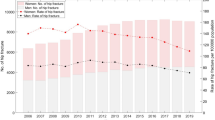
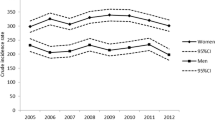
Several studies evaluated hip fracture incidences and its predictors and trends using hospital discharge registries. However, this source does not provide patient-related data, therefore the hospital changes or re-hospitalisations cannot be identified as “double counting”. If double counting differs with age, sex, region, and time, the estimates may be biased. Aim of our study was to evaluate the magnitude of multiple counting and, in particular, its variation with age, sex, region, and calendar year. We used data of a German-wide health insurance (1.6 million members). Between 1998 and 2009, we assessed all hip fractures (ICD 9: 820, ICD 10: S.72.0–2) in individuals aged 50 years or older and calculated the probability to be a patient’s “first” fracture in each calendar year. Using multiple logistic regressions, we estimated the influence of age, sex, region, and calendar year. The probabilities of a “first fracture” per patient and year varied between 86.7 % (95 % confidence interval 83.9–89.2 %, year 2003) and 93.9 % (90.9–96.2 %, year 1998). Age (odds ratio per 5 years 0.89; 95 % CI 0.86–0.92), region (East vs. West Germany: 0.65; 0.52–0.81), and calendar year (per year 0.97; 0.95–0.99) were significantly associated in the multiple regression. The probability to have multiple counting of hip fracture events varied significantly with age, region, and calendar year. It should be discussed that analyses which do not account for this may provide invalid estimates and conclusions when differences between age groups and regions or trends are analyzed.
Zusammenfassung
Einige Studien zur Schätzung der Hüftfrakturinzidenz, ihrer Prädiktoren und Trends basieren auf Analysen der Krankenhausdiagnosestatistik. Diese Datenquelle liefert jedoch keine patientenbezogenen Daten, so dass zum Beispiel Verlegungen oder Wiederaufnahmen nicht als Doppelregistrierungen identifiziert werden können. Unterscheiden sich Doppelregistrierungen nach Alter, Geschlecht, Region und Zeit, kann das zu Verzerrungen der Schätzung führen. Ziel unserer Studie war es, das Ausmaß von Mehrfachregistrierungen und insbesondere die Unterschiede nach Alter, Geschlecht, Region und Kalenderjahr abzuschätzen. Wir nutzten Daten einer bundesweiten gesetzlichen Krankenkasse (1,6 Millionen Mitglieder). Für die Jahre 1998–2009 werteten wir alle Hüftfrakturen (ICD 9: 820, ICD 10: S.72,0–2) von Patienten über 50 Jahre und älter aus und schätzten die Zahl der „ersten Hüftfrakturen“ in jedem Kalenderjahr. Unter Nutzung multipler logistischer Regressionen schätzten wir den Einfluss von Alter, Geschlecht, Region und Kalenderjahr. Die Wahrscheinlichkeiten einer „ersten Fraktur“ pro Patient und Jahr variierten zwischen 86,7 % (95 % Konfidenzintervall 83,9–89,2 %, Jahr 2003) und 93,9 % (90,9–96,2, Jahr 1998). Alter (odds ratio pro 5 Jahren 0,89; 95 % CI 0,86–0,92), Region (Ost- vs. Westdeutschland: 0,65; 0,52–0,81) und Kalenderjahr (pro Jahr 0,97; 0,95–0,99) waren in der multiplen Regression signifikant assoziiert. Die Wahrscheinlichkeit, Hüftfrakturen mehrfach zu registrieren, variierte signifikant mit Alter, Region und Kalenderjahr. Es ist zu diskutieren, dass Analysen, die dies nicht berücksichtigen, falsche Schätzungen und Schlussfolgerungen hinsichtlich der analysierten Unterschiede zwischen Altersgruppen und Regionen oder Trends liefern.
Similar content being viewed by others

References
Gullberg B, Johnell O, Kanis JA. Worldwide projections for hip fracture. Osteoporos Int 1997;7:407–413.
Kannus P, Parkkari J, Sievanen H, Heinonen A, Vuori I, Jarvinen M. Epidemiology of hip fractures. Bone 1996;18:57–63.
Barbier S, Ecochard R, Schott AM, Colin C, Delmas PD, Jaglal SB, et al. Geographical variations in hip fracture for women: strong effects hidden in standardised ratios. Osteoporosis Int 2009;20(3):371–377.
Kannus P, Niemi S, Parkkari J, Palvanan M, Vuori I, Jarvinen M. Nationwide decline in incidence of hip fracture. J Bone Mineral Res 2006;21:1836–1838.
Lönnroos E, Kautiainen H, Karppi P, Huusko T, Hartikainen S, Kiviranta I, et al. Increased incidence of hip fractures. A population based study in Finland. Bone 2006;39:623–627.
Giversen IM. Time trends of age-adjusted incidence rates of first hip fractures: a register-based study among older people in Viborg County, Denmark, 1987–1997. Osteoporos Int 2006;17:552–564.
Jaglal SB, Weller I, Mamdani M, Hawker G, Kreder H, Jaakkimainen L, et al. Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res 2005;20:898–905.
Hernandez JL, Olmos JM, Alonso MA, Gonzalez-Fernandez CR, Martinez J, Pajaron M, et al. Trend in hip fracture epidemiology over a 14-year period in a Spanish population. Osteoporos Int 2006;17:464–470.
Löfmann O, Berglund K, Larsson L, Toss G. Changes in hip fracture epidemiology: redistribution between ages, genders, and fracture types. Osteoporos Int 2002;13:18–25.
Centers for Disease Control and Prevention. Fatalities and injuries from falls among older adults—United States, 1993–2003 and 2001–2005. Morb Mortal Wkly Rep 2006;55:1221–1224.
Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R. Incidence of hip fracture over a 10-year period (1991–2000): reversal of a secular trend. Bone 2007;40:1284–1289.
Mann E, Icks A, Haastert B, Meyer G. Hip fracture incidence in the elderly in Austria: an epidemiological study covering the years 1994–2006. BMC Geriatr 2008;8:35.
Icks A, Haastert B, Wildner C, Becker C, Meyer G. Trend of hip fracture incidence in Germany 1995–2004: a population based study. Osteoporos Int 2008;19:1139–1145.
Icks A, Haastert B, Wildner M, Becker C, Rapp K, Dragano N, et al. Hip fractures and area level socioeconomic conditions. A population-based study. BMC Public Health 2009;9:114.
Leslie WD, O’Donnell S, Jean S, Lagace C, Walsh P, Bancej C, et al. For the Osteoporosis Surveillance Expert Working Group: trends in hip fracture rates in Canada. JAMA 2009;302(8):883–889.
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA 2009;302(14):1573–1579.
Wildner M, Clark DE. Hip fracture incidence in East and West Germany. Reassessment 10 years after unification. Osteoporos Int 2001;12:136–139.
Hoffmann F, Glaeske G. Incidence of proximal femur fractures in Germany. Individual-based analysis of a statutory health insurance‘ population. Gesundheitswesen 2006;68:161–164.
Dimai HP, Svedbom A, Fahrleitner-Pammer A, Pieber T, Resch H, Zwettler E, et al. Epidemiology of hip fractures in Austria: evidence for a change in the secular trend. Osteoporos Int 2010;22(2):685–92.
Schnee M. Sozioökonomische Strukturen und Morbidität in den gesetzlichen Krankenkassen. In: Böcken J, Braun B, Amhof R, editors. Gesundheitsmonitor 2008. Gütersloh: Verlag Bertelsmann Stiftung: 2008;88–104.
Mann E, Icks A, Haastert B, Meyer G. Letter to the Editor. Wien Klin Wochenschr 2010,122(17–18):545.
Acknowledgments
We would like to thank Olaf Schoffer from the Federal Statistical Office, Wiesbaden (Research Data Center, Kamen and Dresden). We further thank the Gmünder ErsatzKasse (GEK) for providing the data and for supporting us in data management. The study was supported by a grant from the North-Rhine Westphalian Ministry of Health and Social Services.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Icks, A., Haastert, B., Glaeske, G. et al. Correction factor for the analysis of the hip fracture incidence—differences between age, sex, region, and calendar year. Wien Klin Wochenschr 124, 391–394 (2012). https://doi.org/10.1007/s00508-012-0188-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-012-0188-z