
Abstract
Background
The purpose of this study was to evaluate long-term prognosis and cause of death in patients with superficial esophageal adenocarcinoma (SEAC) after surgery.
Patients and Methods
A total of 85 patients without adjuvant or neoadjuvant treatment underwent surgery for SEAC (pT1N0–1, M0) 1984–2011. Medical records and causes of death were reviewed, and 79 specimens (93 %) were reanalyzed for cancer penetration. Survival was calculated according to Kaplan–Meier and comparisons of survival with log-rank test. Multivariate survival was analyzed with Cox proportional hazards model.
Results
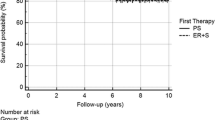
Of 85 patients, 36 had transhiatal, 33 transthoracic en bloc, 6 minimally invasive en bloc, 5 vagal sparing esophageal resection and 5 endoscopic mucosal resections; 7 patients (8 %) had lymph node metastasis (LNM). Cancer penetration: 35 pT1a and 44 pT1b. Overall survival was 67 % at 5 years and 50 % at 10 years. Disease-specific survival was 82 % at 5 years and 78 % at 10 years. Recurrence-free survival was 80 % at 5 years. In a Cox multivariate model, poor overall survival was predicted only by LNM. Cumulative mortality during median follow-up of 5 years (0–25 years): 37 of 85 (44 %). Cause of death of these 37: SEAC recurrence for 15 (41 %), postoperative complications for 4 (11 %), another primary malignancy for 5 (14 %), non-cancer-related for 11 (30 %) and for 2 (5 %) cause unknown. Mortality after 5-year follow-up: 11 (30 %); 82 % of these deaths were unrelated to SEAC recurrence.
Conclusions
With SEAC recurrence as the single most common cause of death, disease-specific 5-year survival was good. Overall and late (> 5-year) survival is affected by diseases related to aging.

Similar content being viewed by others

References
Sihvo EI, Luostarinen ME, Salo JA. Fate of patients with adenocarcinoma of the esophagus and the esophagogastric junction: a population-based analysis. Am J Gastroenterol. 2004;99:419–24.
Tachibana M, Kinugasa S, Shibakita M, Tonomoto Y, Hattori S, Hyakudomi R, et al. Surgical treatment of superficial esophageal cancer. Langenbecks Arch Surg. 2006;391:304–21.
Spechler SJ. Barrett’s esophagus: clinical issues. Gastrointest Endosc Clin N Am. 2011;21:1–7.
Dent J. Barrett’s esophagus: a historical perspective, an update on core practicalities and predictions on future evolutions of management. J Gastroenterol Hepatol. 2011;26 Suppl 1:11–30.
Menke-Pluymers MB, Schoute NW, Mulder AH, Hop WC, van Blankenstein M, Tilanus HW. Outcome of surgical treatment of adenocarcinoma in Barrett’s oesophagus. Gut. 1992;33:1454–8.
Holscher AH, Bollschweiler E, Schneider PM, Siewert JR. Prognosis of early esophageal cancer. Comparison between adeno- and squamous cell carcinoma. Cancer. 1995;76:178–86.
Ruol A, Parenti A, Zaninotto G, Merigliano S, Costantini M, Cagol M, et al. Intestinal metaplasia is the probable common precursor of adenocarcinoma in barrett esophagus and adenocarcinoma of the gastric cardia. Cancer. 2000;88:2520–8.
Rice TW, Blackstone EH, Goldblum JR, DeCamp MM, Murthy SC, Falk GW, et al. Superficial adenocarcinoma of the esophagus. J Thorac Cardiovasc Surg. 2001;122:1077–90.
van Sandick JW, van Lanschot JJ, ten Kate FJ, Offerhaus GJ, Fockens P, Tytgat GN, et al. Pathology of early invasive adenocarcinoma of the esophagus or esophagogastric junction: implications for therapeutic decision making. Cancer. 2000;88:2429–37.
Leers JM, DeMeester SR, Oezcelik A, Klipfel N, Ayazi S, Abate E, et al. The prevalence of lymph node metastases in patients with T1 esophageal adenocarcinoma a retrospective review of esophagectomy specimens. Ann Surg. 2011;253:271–8.
Stein HJ, Feith M, Mueller J, Werner M, Siewert JR. Limited resection for early adenocarcinoma in Barrett’s esophagus. Ann Surg. 2000;232:733–42.
Sepesi B, Watson TJ, Zhou D, Polomsky M, Litle VR, Jones CE, et al. Are endoscopic therapies appropriate for superficial submucosal esophageal adenocarcinoma? An analysis of esophagectomy specimens. J Am Coll Surg. 2010;210:418–27.
Ancona E, Rampado S, Cassaro M, Battaglia G, Ruol A, Castoro C, et al. Prediction of lymph node status in superficial esophageal carcinoma. Ann Surg Oncol. 2008;15:3278–88.
Westerterp M, Koppert LB, Buskens CJ, Tilanus HW, ten Kate FJ, Bergman JJ, et al. Outcome of surgical treatment for early adenocarcinoma of the esophagus or gastro-esophageal junction. Virchows Arch. 2005;446:497–504.
Cen P, Hofstetter WL, Correa AM, Wu TT, Lee JH, Ross WA, et al. Lymphovascular invasion as a tool to further subclassify T1b esophageal adenocarcinoma. Cancer. 2008;112:1020–7.
Liu L, Hofstetter WL, Rashid A, Swisher SG, Correa AM, Ajani JA, et al. Significance of the depth of tumor invasion and lymph node metastasis in superficially invasive (T1) esophageal adenocarcinoma. Am J Surg Pathol. 2005;29:1079–85.
Institute for Algorithmic Medicine. A Texas Non-profit Corporation. 01.13-01 Comorbidity Index and Score of Charlson et al. Purpose: To use the comorbidity score developed by Charlson et al. To give an estimate of 10-year survival for a patient. http://www.medal.org/OnlineCalculators/ch1/ch1.13/ch1.13.01.php.
Japanese Society for Esophageal Disease. Guidelines for the clinical and pathological studies on carcinoma of the esophagus. Jpn J Surg. 1976;6:69–78.
Holscher AH, Bollschweiler E, Schroder W, Metzger R, Gutschow C, Drebber U. Prognostic impact of upper, middle, and lower third mucosal or submucosal infiltration in early esophageal cancer. Ann Surg. 2011;254:802–7; discussion 807–8.
Rizk N, Venkatraman E, Park B, Flores R, Bains MS, Rusch V. The prognostic importance of the number of involved lymph nodes in esophageal cancer: implications for revisions of the American Joint Committee on Cancer staging system. J Thorac Cardiovasc Surg. 2006;132:1374–81.
Stein HJ, Feith M, Bruecher BL, Naehrig J, Sarbia M, Siewert JR. Early esophageal cancer: pattern of lymphatic spread and prognostic factors for long-term survival after surgical resection. Ann Surg. 2005;242:566–73; discussion 573–5.
Ruol A, Merigliano S, Baldan N, Santi S, Petrin GF, Bonavina L, et al. Prevalence, management and outcome of early adenocarcinoma (pT1) of the esophago-gastric junction. Comparison between early cancer in Barrett’s esophagus (type I) and early cancer of the cardia (type II). Dis Esophagus. 1997;10:190–5.
Christein JD, Hollinger EF, Millikan KW. Prognostic factors associated with resectable carcinoma of the esophagus. Am Surg. 2002;68:258–62; discussion 262–3.
Rice TW, Blackstone EH, Adelstein DJ, Zuccaro G Jr, Vargo JJ, Goldblum JR, et al. N1 esophageal carcinoma: the importance of staging and downstaging. J Thorac Cardiovasc Surg. 2001;121:454–64.
Gockel I, Domeyer M, Sgourakis GG, Schimanski CC, Moehler M, Kirkpatrick CJ, et al. Prediction model of lymph node metastasis in superficial esophageal adenocarcinoma and squamous cell cancer including D2-40 immunostaining. J Surg Oncol. 2009;100:191–8.
Cen P, Banki F, Cheng L, Khalil K, Du XL, Fallon M, et al. Changes in age, stage distribution, and survival of patients with esophageal adenocarcinoma over three decades in the United States. Ann Surg Oncol. 2012;19:1685–91.
Bollschweiler E, Baldus SE, Schroder W, Prenzel K, Gutschow C, Schneider PM, et al. High rate of lymph-node metastasis in submucosal esophageal squamous-cell carcinomas and adenocarcinomas. Endoscopy. 2006;38:149–56.
Rudiger Siewert J, Feith M, Werner M, Stein HJ. Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg. 2000;232:353–61.
Omloo JM, Lagarde SM, Hulscher JB, Reitsma JB, Fockens P, van Dekken H, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg. 2007;246:992–1000; discussion 1000–1.
Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–9.
Bennett C, Vakil N, Bergman J, Harrison R, Odze R, Vieth M, et al. Consensus statements for management of Barrett’s dysplasia and early-stage esophageal adenocarcinoma, based on a Delphi process. Gastroenterology. 2012;143:336–46.
Acknowledgment
The authors thank Mrs. Yvonne Sundström for her skillful technical and secretarial assistance. This study was supported by Helsinki University Central Hospital Research Funds (EVO). Professor Jarmo Salo had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Conflict of interest
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kauppi, J., Gockel, I., Rantanen, T. et al. Cause of Death During Long-Term Follow-up for Superficial Esophageal Adenocarcinoma. Ann Surg Oncol 20, 2428–2433 (2013). https://doi.org/10.1245/s10434-013-2866-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-2866-0